

Case Reports
doi: 10.4061/2010/950524.
Lower body positive pressure application with an antigravity suit in acute carotid occlusion
Affiliations
- PMID: 20798842
- PMCID: PMC2925369
- DOI: 10.4061/2010/950524
Item in Clipboard
Case Reports
Lower body positive pressure application with an antigravity suit in acute carotid occlusion
Stroke Res Treat.
.
Abstract
The challenge in acute stroke is still to reperfuse as early as possible the ischemic territory. Since fibrinolytic therapies have a limited window with potential risk of bleeding, having a nonpharmacologic mean to recruit vessels in area surrounding necrosis might be useful. We propose here to use antigravity suit inflated at "venous" pressure levels to shift blood towards thoracic and brain territories. We report two cases of spectacular clinical recovery after acute carotid occlusion.
Figures
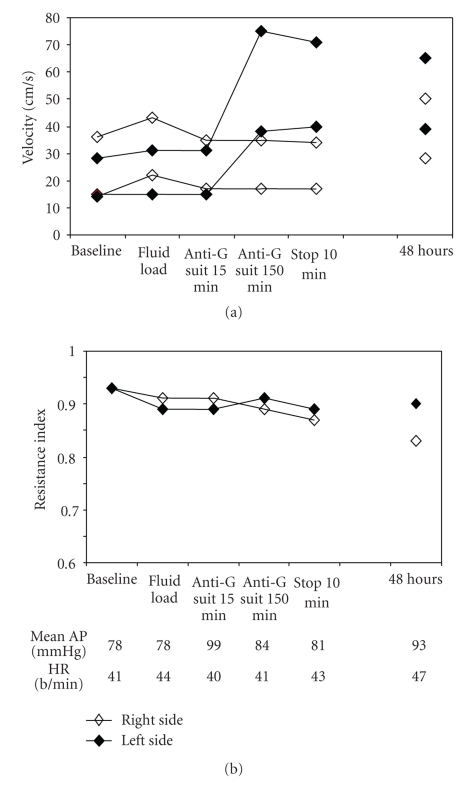
(a) Patterns of intracranial MCA blood flow velocities with time in both the right and left sides, before, during, and after (10 minutes and 48 hours) LBPP application. Note the left side improvement in systolic and diastolic blood flow velocity induced by LBPP, which was sustained for at least 2 days. (b) Vascular resistance index (RI) evolution (method for computation: systolic V/diastolic V). A clear difference between right and left RI occurred only after 48 hours of LBPP application. Corresponding mean arterial pressure (mean AP) and heart rate (HR) at each time.
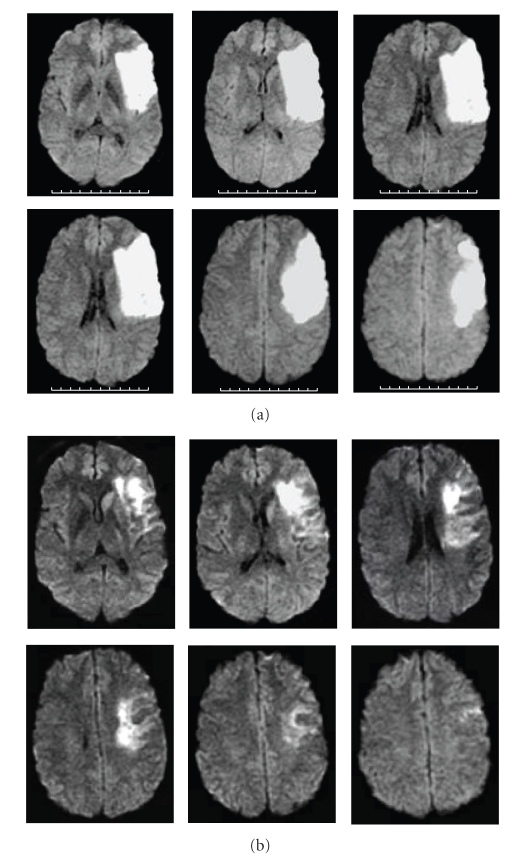
MRI diffusion-weighted images showing left superficial MCA infarct. (a) 24 hours after stroke onset, (b) 5 days after stroke onset.
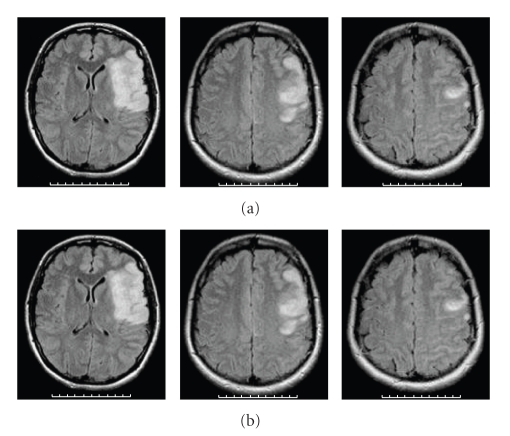
MRI T2 flair-weighted images showing left superficial MCA infarct. (a) 24 hours after stroke onset, (b) 5 days after stroke onset.
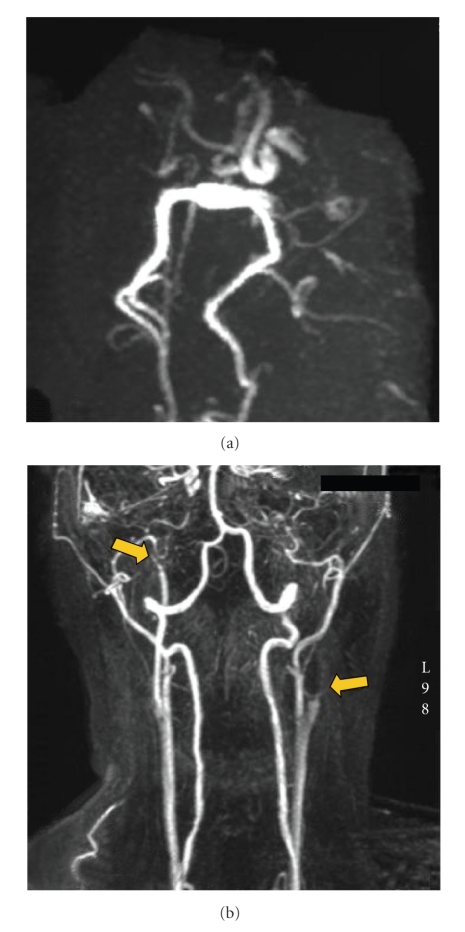
(a) Intracranial MRA of Willis circle: right siphon, right and left MCAs were not visible. Posterior communicating arteries were also not visible, with visible posterior cerebral arteries. (b) Cervical MRA showing proximal left internal carotid artery occlusion and distal right internal carotid artery tight stenosis (arrows).
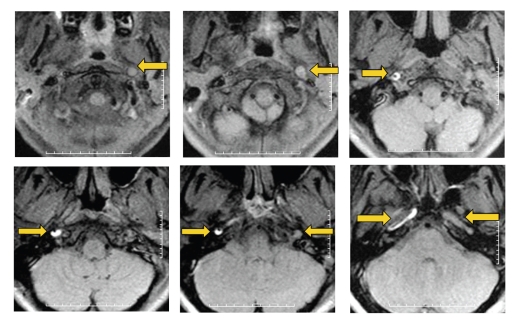
MRI T1-FAT-SAT-weighted images showing the dissecting process visible as a hypersignal in the wall of both ICAs as well as an enhancement of ICA diameter (arrows).
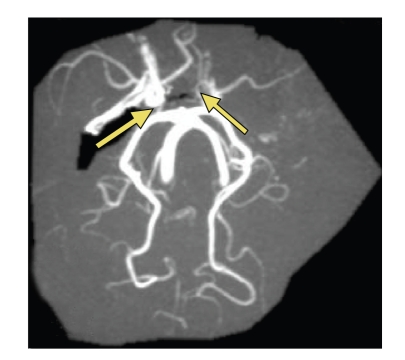
Intracranial MRA showing recanalisation of the right ICA; the right and left MCAs are visible as well as both posterior communicating arteries (arrows).
Similar articles
-
[Maximal exercise in spinal cord injured subjects: effects of an antigravity suit].Sci Sports. 1996;11(3):173-9. doi: 10.1016/0765-1597(96)84030-5. Sci Sports. 1996. PMID: 11541516 French.
-
The antigravity suit in neurosurgery. Cardiovascular responses in seated neurosurgical patients.Anaesthesia. 1988 Sep;43(9):762-5. doi: 10.1111/j.1365-2044.1988.tb05751.x. Anaesthesia. 1988. PMID: 3052159
-
Endovascular recanalization of internal carotid artery occlusion in acute ischemic stroke.AJNR Am J Neuroradiol. 2005 Nov-Dec;26(10):2591-4. AJNR Am J Neuroradiol. 2005. PMID: 16286407 Free PMC article.
-
Management of carotid near-occlusion and acute carotid occlusion.J Cardiovasc Surg (Torino). 2016 Apr;57(2):145-51. Epub 2015 Dec 16. J Cardiovasc Surg (Torino). 2016. PMID: 26675835 Review.
-
Treatment Strategies for Acute Ischemic Stroke Caused by Carotid Artery Occlusion.Interv Neurol. 2016 Sep;5(3-4):148-156. doi: 10.1159/000445304. Epub 2016 Jun 28. Interv Neurol. 2016. PMID: 27781043 Free PMC article. Review.
Cited by
-
Partial aortic occlusion and cerebral venous steal: venous effects of arterial manipulation in acute stroke.Stroke. 2011 May;42(5):1478-81. doi: 10.1161/STROKEAHA.110.603852. Epub 2011 Mar 24. Stroke. 2011. PMID: 21441149 Free PMC article.
-
The Concept of Venous Steal: The Impact of Vascular Stenosis and Outflow Pressure Gradient on Blood Flow Diversion.Medicina (Kaunas). 2025 Apr 6;61(4):672. doi: 10.3390/medicina61040672. Medicina (Kaunas). 2025. PMID: 40282963 Free PMC article. Review.
References
-
- Frank LR. Is MAST in the past? The pros and cons of MAST usage in the field. Journal of Emergency Medical Services. 2000;25(2):38–41, 44–45. - PubMed
-
- McSwain N. Pneumatic anti-shock garment in the ’90s. Emergency. 1994;26(4):53–56.
-
- Payen DM, Brun-Buisson CJL, Carli PA, et al. Hemodynamic, gas exchange, and hormonal consequences of LBPP during PEEP ventilation. Journal of Applied Physiology. 1987;62(1):61–70. - PubMed
-
- Payen DM, Carli PA, Brun-Buisson CJL, et al. Lower body positive pressure vs. dopamine during PEEP in humans. Journal of Applied Physiology. 1985;58(1):77–82. - PubMed
-
- Wojner-Alexandrov AW, Garami Z, Chernyshev OY, Alexandrov AV. Heads down: flat positioning improves blood flow velocity in acute ischemic stroke. Neurology. 2005;64(8):1354–1357. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
