

Molecular epidemiology of a hepatitis C virus epidemic in a haemodialysis unit: outbreak investigation and infection outcome
- PMID: 20799943
- PMCID: PMC2940904
- DOI: 10.1186/1471-2334-10-257
Molecular epidemiology of a hepatitis C virus epidemic in a haemodialysis unit: outbreak investigation and infection outcome
Abstract
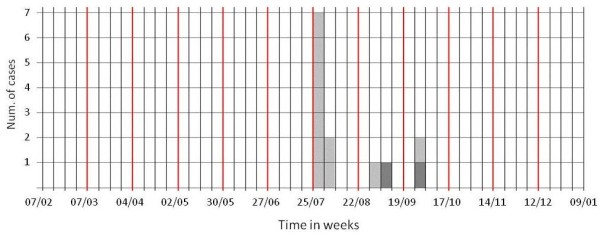
Background: HCV is a leading cause of liver chronic diseases all over the world. In developed countries the highest prevalence of infection is reported among intravenous drug users and haemodialysis (HD) patients. The present report is to identify the pathway of HCV transmission during an outbreak of HCV infection in a privately run haemodialysis (HD) unit in Italy in 2005.
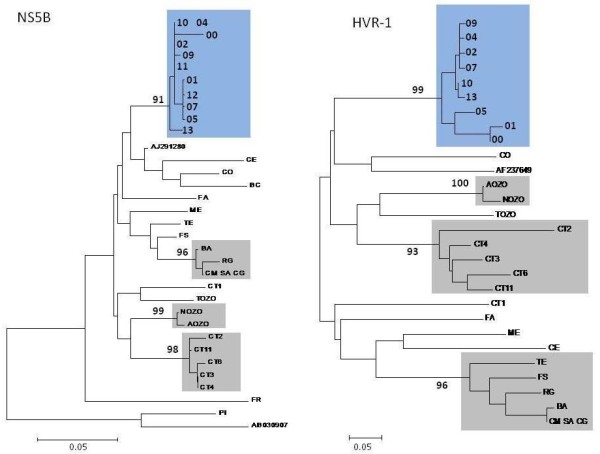
Methods: Dynamics of the outbreak and infection clinical outcomes were defined through an ambi-directional cohort study. Molecular epidemiology techniques were used to define the relationships between the viral variants infecting the patients and confirm the outbreak. Risk analysis and auditing procedures were carried out to define the transmission pathway(s).
Results: Of the 50 patients treated in the HD unit 5 were already anti-HCV positive and 13 became positive during the study period (AR = 28.9%). Phylogenic analysis identified that, all the molecularly characterized incident cases (10 out of 13), were infected with the same viral variant of one of the prevalent cases. The multivariate analysis and the auditing procedure disclosed a single event of multi-dose vials heparin contamination as the cause of transmission of the infection in 11 out of the 13 incident cases; 2 additional incident cases occurred possibly as a result of inappropriate risk management.
Discussion: More than 30% of all HCV infections in developed countries results from poor application of standard precautions during percutaneous procedures. Comprehensive strategy which included: educational programmes, periodical auditing on standard precaution, use of single-dose vials whenever possible, prospective surveillance for blood-borne infections (including a system of prompt notification) and risk assessment/management dedicated staff are the cornerstone to contain and prevent outbreaks in HD CONCLUSIONS: The outbreak described should serve as a reminder to HD providers that patients undergoing dialysis are at risk for HCV infection and that HCV may be easily transmitted whenever standard precautions are not strictly applied.
Figures
References
-
- Jadoul M, Poignet JL, Geddes C, Locatelli F, Medin C, Krajewska M, Barril G, Scheuermann E, Sonkodi S, Goubau P. the HCV Collaborative Group. The changing epidemiology of hepatitisCvirus (HCV) infection in haemodialysis: European multicentre study. Nephrol Dial Transplant. 2004;19:904–909. doi: 10.1093/ndt/gfh012. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
