

Early identification of patients at risk of acute lung injury: evaluation of lung injury prediction score in a multicenter cohort study
- PMID: 20802164
- PMCID: PMC3056224
- DOI: 10.1164/rccm.201004-0549OC
Early identification of patients at risk of acute lung injury: evaluation of lung injury prediction score in a multicenter cohort study
Abstract
Rationale: Accurate, early identification of patients at risk for developing acute lung injury (ALI) provides the opportunity to test and implement secondary prevention strategies.
Objectives: To determine the frequency and outcome of ALI development in patients at risk and validate a lung injury prediction score (LIPS).
Methods: In this prospective multicenter observational cohort study, predisposing conditions and risk modifiers predictive of ALI development were identified from routine clinical data available during initial evaluation. The discrimination of the model was assessed with area under receiver operating curve (AUC). The risk of death from ALI was determined after adjustment for severity of illness and predisposing conditions.
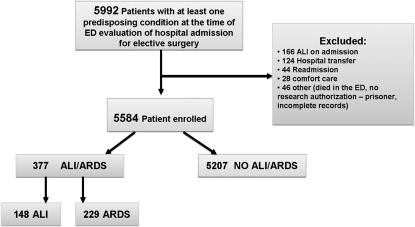
Measurements and main results: Twenty-two hospitals enrolled 5,584 patients at risk. ALI developed a median of 2 (interquartile range 1-4) days after initial evaluation in 377 (6.8%; 148 ALI-only, 229 adult respiratory distress syndrome) patients. The frequency of ALI varied according to predisposing conditions (from 3% in pancreatitis to 26% after smoke inhalation). LIPS discriminated patients who developed ALI from those who did not with an AUC of 0.80 (95% confidence interval, 0.78-0.82). When adjusted for severity of illness and predisposing conditions, development of ALI increased the risk of in-hospital death (odds ratio, 4.1; 95% confidence interval, 2.9-5.7).
Conclusions: ALI occurrence varies according to predisposing conditions and carries an independently poor prognosis. Using routinely available clinical data, LIPS identifies patients at high risk for ALI early in the course of their illness. This model will alert clinicians about the risk of ALI and facilitate testing and implementation of ALI prevention strategies. Clinical trial registered with www.clinicaltrials.gov (NCT00889772).
Figures



References
-
- The ARDS Network. Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2000;283:1995–2002. - PubMed
-
- Jepsen S, Herlevsen P, Knudsen P, Bud MI, Klausen NO. Antioxidant treatment with N-acetylcyesteine during adult respiratory distress syndrome: a prospective randomized placebo controlled study. Crit Care Med 1992;20:819–823. - PubMed
-
- Meade MO, Jacka MJ, Cook DJ, Dodek P, Griffith L, Guyatt GH. Survey of interventions for the prevention and treatment of acute respiratory distress syndrome. Crit Care Med 2004;32:946–954. - PubMed
-
- The ARDS Clinical Trials Network. Randomized, placebo-controlled trial of lisofylline for early treatment of acute lung injury and acute respiratory distress syndrome. Crit Care Med 2002;30:1–6. - PubMed
-
- Zeiher BG, Artigas A, Vincent JL, Dmitrienko A, Jackson K, Thompson BT, Bernard G; STRIVE Study Group. Neutrophil elastase inhibition in acute lung injury: results of the STRIVE study. Crit Care Med 2004;32:1695–1702. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
