

High prevalence of normal tests assessing hypercortisolism in subjects with mild and episodic Cushing's syndrome suggests that the paradigm for diagnosis and exclusion of Cushing's syndrome requires multiple testing
- PMID: 20803415
- PMCID: PMC2978784
- DOI: 10.1055/s-0030-1263128
High prevalence of normal tests assessing hypercortisolism in subjects with mild and episodic Cushing's syndrome suggests that the paradigm for diagnosis and exclusion of Cushing's syndrome requires multiple testing
Abstract
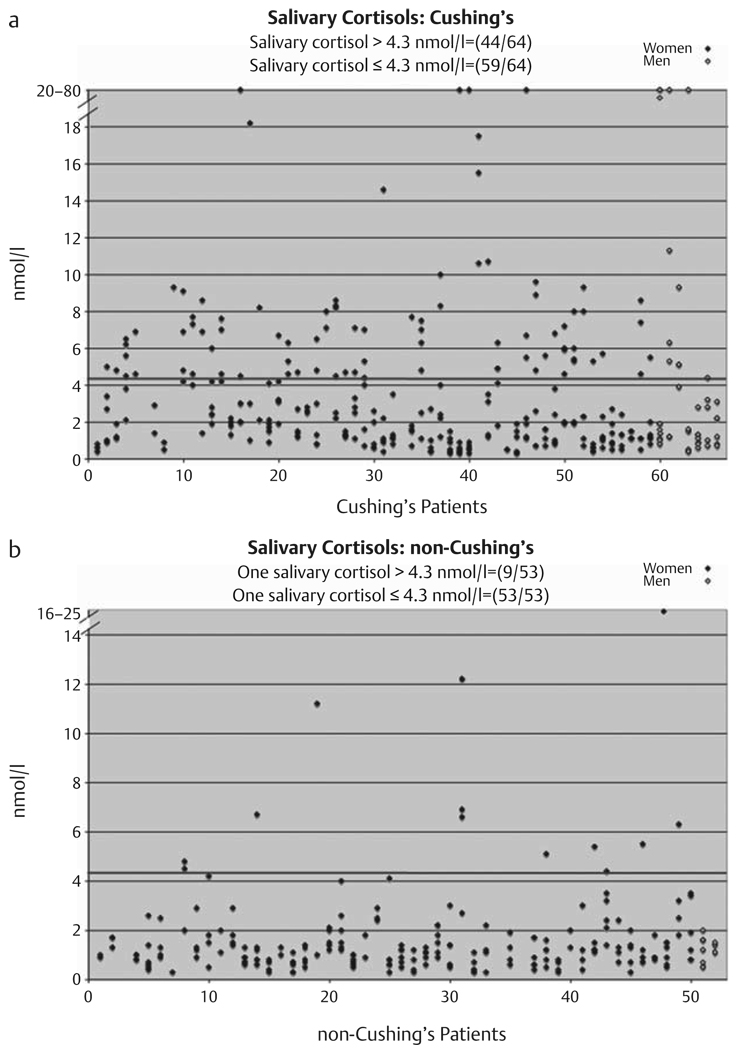
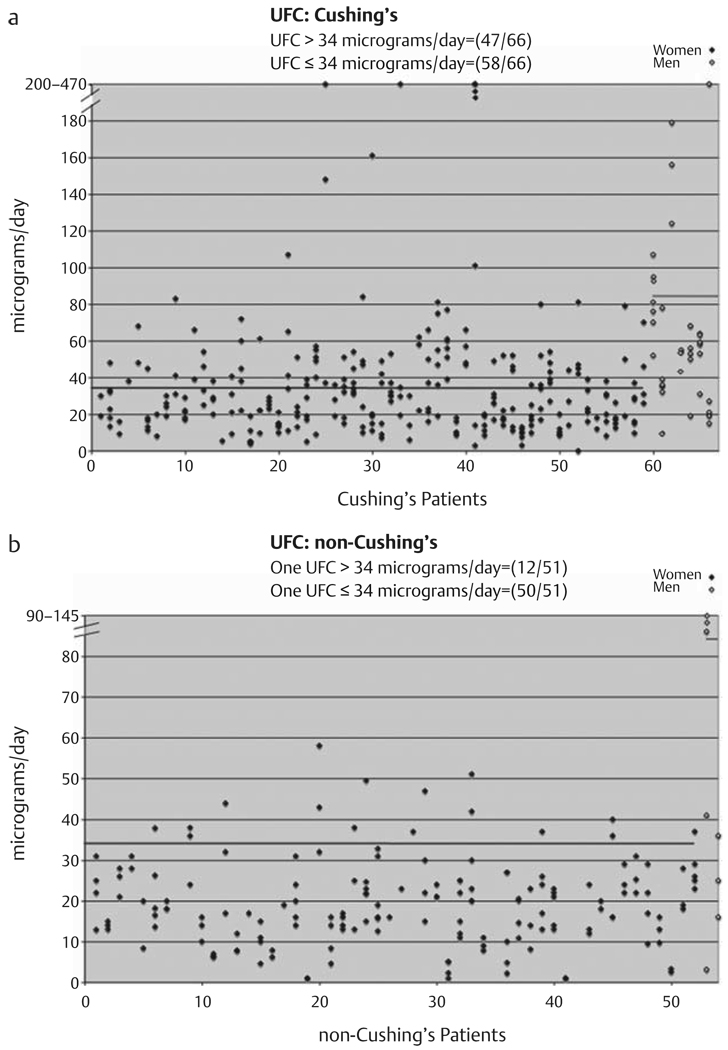
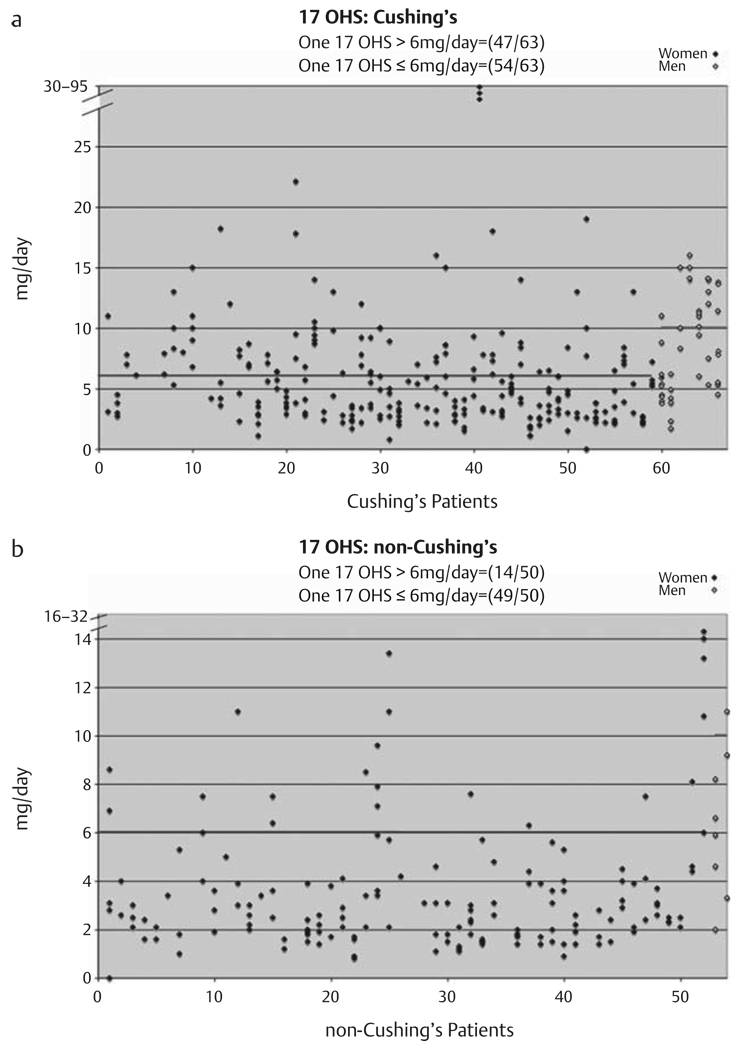
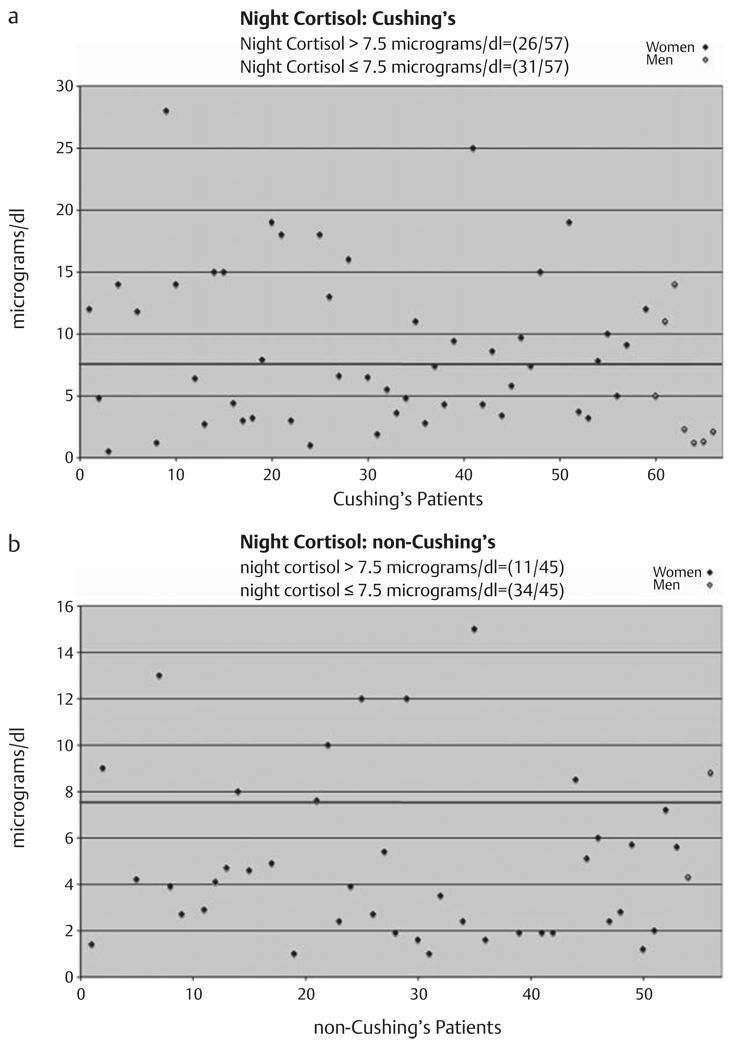
Many Endocrinologists believe that a single determination of eucortisolism or a single demonstration of appropriate suppression to dexamethasone excluded Cushing's syndrome, except in what was previously thought to be the rare patient with episodic or periodic Cushing's syndrome. We hypothesize that episodic Cushing's syndrome is relatively common and a single test assessing hypercortisolism may not be sufficient to accurately rule out or diagnose Cushing's syndrome and retrospectively examined the number of normal and abnormal tests assessing hypercortisolism performed on multiple occasions in 66 patients found to have mild and/or episodic Cushing's syndrome compared to a similar group of 54 patients evaluated for, but determined not to have Cushing's syndrome. We found that 65 of the 66 patients with Cushing's syndrome had at least one normal test of cortisol status and most patients had several normal tests. The probability of having Cushing's syndrome when one test was negative was 92% for 23:00 h salivary cortisol, 88% for 24-h UFC, 86% for 24-h 17OHS, and 54% for nighttime plasma cortisol. These results demonstrated that episodic hypercortisolism is highly prevalent in subjects with mild Cushing's syndrome and no single test was effective in conclusively diagnosing or excluding the condition. Rather, the paradigm for the diagnosis should be a careful history and physical examination and in those patients in whom mild Cushing's syndrome/disease is strongly suspected, multiple tests assessing hypercortisolism should be performed on subsequent occasions, especially when the patient is experiencing signs and symptoms of short-term hypercortisolism.
© Georg Thieme Verlag KG Stuttgart · New York.
Figures
Similar articles
-
Late-night salivary cortisol as a screening test for Cushing's syndrome.J Clin Endocrinol Metab. 1998 Aug;83(8):2681-6. doi: 10.1210/jcem.83.8.4936. J Clin Endocrinol Metab. 1998. PMID: 9709931
-
Midnight salivary cortisol for the initial diagnosis of Cushing's syndrome of various causes.J Clin Endocrinol Metab. 2004 Jul;89(7):3345-51. doi: 10.1210/jc.2003-031790. J Clin Endocrinol Metab. 2004. PMID: 15240613 Clinical Trial.
-
An update on the overnight dexamethasone suppression test for the diagnosis of Cushing's syndrome: limitations in patients with mild and/or episodic hypercortisolism.Exp Clin Endocrinol Diabetes. 2006 Jul;114(7):356-60. doi: 10.1055/s-2006-924281. Exp Clin Endocrinol Diabetes. 2006. PMID: 16915537
-
[Cushing's syndrome: diagnostic exploration].Presse Med. 1994 Jan 8-15;23(1):43-8. Presse Med. 1994. PMID: 8127815 Review. French.
-
Pitfalls in the diagnosis and management of Cushing's syndrome.Neurosurg Focus. 2015 Feb;38(2):E4. doi: 10.3171/2014.11.FOCUS14704. Neurosurg Focus. 2015. PMID: 25639322 Review.
Cited by
-
Cyclic Subclinical Hypercortisolism: A Previously Unidentified Hypersecretory Form of Adrenal Incidentalomas.J Endocr Soc. 2019 Feb 11;3(3):678-686. doi: 10.1210/js.2018-00385. eCollection 2019 Mar 1. J Endocr Soc. 2019. PMID: 30854503 Free PMC article.
-
Cushing's Syndrome in a Patient With Rathke's Cleft Cyst and ACTH Cell Hyperplasia Detected by 11C-Methionine PET Imaging-A Case Presentation.Front Endocrinol (Lausanne). 2020 Jul 22;11:460. doi: 10.3389/fendo.2020.00460. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32774326 Free PMC article.
-
High Prevalence of Adrenal Remnant Tissue in Patients Undergoing Bilateral Adrenalectomy for Cushing's Disease.Horm Metab Res. 2021 Mar;53(3):161-168. doi: 10.1055/a-1253-2854. Epub 2020 Oct 22. Horm Metab Res. 2021. PMID: 33091942 Free PMC article.
-
Low-Dose and Standard Overnight and Low Dose-Two Day Dexamethasone Suppression Tests in Patients with Mild and/or Episodic Hypercortisolism.Horm Metab Res. 2018 Jun;50(6):453-461. doi: 10.1055/a-0603-3868. Epub 2018 May 2. Horm Metab Res. 2018. PMID: 29719879 Free PMC article.
-
Hair cortisol in the evaluation of Cushing syndrome.Endocrine. 2017 Apr;56(1):164-174. doi: 10.1007/s12020-017-1231-7. Epub 2017 Feb 13. Endocrine. 2017. PMID: 28194652 Free PMC article.
References
-
- Newell-Price J, Trainer P, Besser M, Grossman A. The diagnosis and differential diagnosis of Cushing’s syndrome and pseudo-Cushing’s states. Endocr Rev. 1998;19:647–672. - PubMed
-
- Kidambi S, Raff H, Findling JW. Limitations of nocturnal salivary cortisol and urine free cortisol in the diagnosis of mild Cushing’s syndrome. Eur J Endocrinol. 2007;157:725–731. - PubMed
-
- Mantero F, Scaroni CM, Albiger NM. Cyclic Cushing’s syndrome: an overview. Pituitary. 2004;7:203–207. - PubMed
-
- Velez DA, Mayberg MR, Ludlam WH. Cyclic Cushing syndrome: definitions and treatment implications. Neurosurg Focus. 2007;23 E4; discussion E4a. - PubMed
-
- Meinardi JR, Wolffenbuttel BH, Dullaart RP. Cyclic Cushing’s syndrome: a clinical challenge. Eur J Endocrinol. 2007;157:245–254. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
