

Enantioselective pharmacokinetics of (R)- and (S)-ketamine after a 5-day infusion in patients with complex regional pain syndrome
- PMID: 20803495
- PMCID: PMC4701199
- DOI: 10.1002/chir.20890
Enantioselective pharmacokinetics of (R)- and (S)-ketamine after a 5-day infusion in patients with complex regional pain syndrome
Abstract
Introduction: This study determined the pharmacokinetics and pharmacodynamics of (R)- and (S)-ketamine and (R)- and (S)-norketamine following a 5-day moderate dose, as a continuous (R,S)-ketamine infusion in complex regional pain syndrome (CRPS) patients.
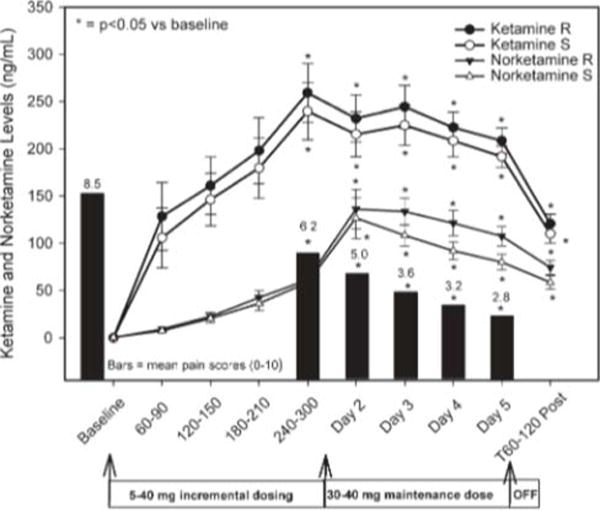
Materials and methods: Ketamine was titrated to 10-40 mg/h and maintained for 5 days. (R)- and (S)-Ketamine and (R)- and (S)-norketamine pharmacokinetic and pharmacodynamic studies were performed. Blood samples were obtained on Day 1 preinfusion, and at 60-90, 120-150, 180-210, and 240-300 min after the start of the infusion, on Days 2, 3, 4, 5, and on Day 5 at 60 min after the end of infusion. The plasma concentrations of (R)- and (S)-ketamine and (R)- and (S)-norketamine were determined using enantioselective liquid chromatography-mass spectrometry.
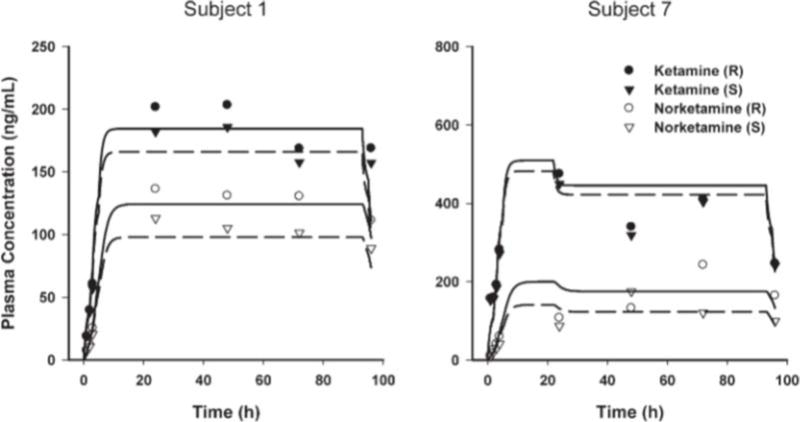
Results: Ketamine and norketamine levels stabilized 5 h after the start of the infusion. (R)-Ketamine clearance was significantly lower resulting in higher steady-state plasma concentrations than (S)-ketamine. The first-order elimination for (S)-norketamine was significantly greater than that of (R)-enantiomer. When comparing the pharmacokinetic parameters of the patients who responded to ketamine treatment with those who did not, no differences were observed in ketamine clearance and the first-order elimination of norketamine.
Conclusion: The results indicate that (R)- and (S)-ketamine and (R)- and (S)-norketamine plasma concentrations do not explain the antinociceptive activity of the drug in patients suffering from CRPS.
Copyright © 2010 Wiley-Liss, Inc.
Figures
Similar articles
-
A parallel chiral-achiral liquid chromatographic method for the determination of the stereoisomers of ketamine and ketamine metabolites in the plasma and urine of patients with complex regional pain syndrome.Talanta. 2010 Oct 15;82(5):1892-904. doi: 10.1016/j.talanta.2010.08.005. Epub 2010 Aug 13. Talanta. 2010. PMID: 20875593 Free PMC article.
-
Pharmacodynamic profiles of ketamine (R)- and (S)- with 5-day inpatient infusion for the treatment of complex regional pain syndrome.Pain Physician. 2010 Jul-Aug;13(4):379-87. Pain Physician. 2010. PMID: 20648207 Free PMC article. Clinical Trial.
-
Pharmacokinetics of ketamine and norketamine enantiomers after racemic or S-ketamine IV bolus administration in dogs during sevoflurane anaesthesia.Res Vet Sci. 2017 Jun;112:208-213. doi: 10.1016/j.rvsc.2017.05.005. Epub 2017 May 6. Res Vet Sci. 2017. PMID: 28521255 Clinical Trial.
-
Ketamine: A Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy.Clin Pharmacokinet. 2016 Sep;55(9):1059-77. doi: 10.1007/s40262-016-0383-6. Clin Pharmacokinet. 2016. PMID: 27028535 Review.
-
Ketamine Infusion for Complex Regional Pain Syndrome Treatment: A Narrative Review.Curr Pain Headache Rep. 2025 Jan 14;29(1):26. doi: 10.1007/s11916-025-01360-9. Curr Pain Headache Rep. 2025. PMID: 39808363 Review.
Cited by
-
A parallel chiral-achiral liquid chromatographic method for the determination of the stereoisomers of ketamine and ketamine metabolites in the plasma and urine of patients with complex regional pain syndrome.Talanta. 2010 Oct 15;82(5):1892-904. doi: 10.1016/j.talanta.2010.08.005. Epub 2010 Aug 13. Talanta. 2010. PMID: 20875593 Free PMC article.
-
Ninety-six hour ketamine infusion with co-administered clonidine for treatment-resistant depression: A pilot randomised controlled trial.World J Biol Psychiatry. 2016 Apr;17(3):230-8. doi: 10.3109/15622975.2016.1142607. Epub 2016 Feb 26. World J Biol Psychiatry. 2016. PMID: 26919405 Free PMC article. Clinical Trial.
-
Stereoselective and regiospecific hydroxylation of ketamine and norketamine.Xenobiotica. 2012 Nov;42(11):1076-87. doi: 10.3109/00498254.2012.685777. Epub 2012 May 21. Xenobiotica. 2012. PMID: 22612619 Free PMC article.
-
Simultaneous population pharmacokinetic modelling of ketamine and three major metabolites in patients with treatment-resistant bipolar depression.Br J Clin Pharmacol. 2012 Aug;74(2):304-14. doi: 10.1111/j.1365-2125.2012.04198.x. Br J Clin Pharmacol. 2012. PMID: 22295895 Free PMC article. Clinical Trial.
-
Subchronic administration of (R,S)-ketamine induces ketamine ring hydroxylation in Wistar rats.J Pharm Biomed Anal. 2016 Aug 5;127:3-8. doi: 10.1016/j.jpba.2016.03.030. Epub 2016 Mar 14. J Pharm Biomed Anal. 2016. PMID: 27017097 Free PMC article.
References
-
- Schwartzman RT, Alexander GM, Grothusen J. Pathophysiology of complex regional pain syndrome. Expert Rev Neurother. 2006;6:669–681. - PubMed
-
- Veldman PH, Goris RJ. Multiple reflex sympathetic dystrophy. Which patients are at risk for developing a recurrence of reflex sympathetic dystrophy in the same or another limb. Pain. 1996;64:463–466. - PubMed
-
- Maleki J, LeBel AA, Bennett GJ, Schwartzman RJ. Patterns of spread in complex regional pain syndrome type I (reflex sympathetic dystrophy) Pain. 2000;88:259–266. - PubMed
-
- Correll GE, Maleki J, Gracely EJ, Muir JJ, Harbut RE. Subanesthetic ketamine infusion therapy: a retrospective analysis of a novel therapeutic approach to complex regional pain syndrome. Pain Med. 2004;5:263–275. - PubMed
-
- Kvarnstrom A, Karlsten R, Quiding H, Emanuelsson BM, Gordh T. The effectiveness of intravenous ketamine and lidocaine on peripheral neuropathic pain. Acta Anaesthesiol Scand. 2003;47:868–877. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
