

Taurine in health and diseases: consistent evidence from experimental and epidemiological studies
- PMID: 20804626
- PMCID: PMC2994368
- DOI: 10.1186/1423-0127-17-S1-S6
Taurine in health and diseases: consistent evidence from experimental and epidemiological studies
Abstract
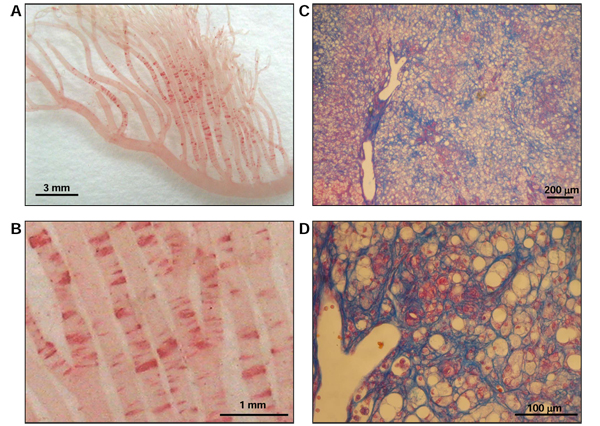
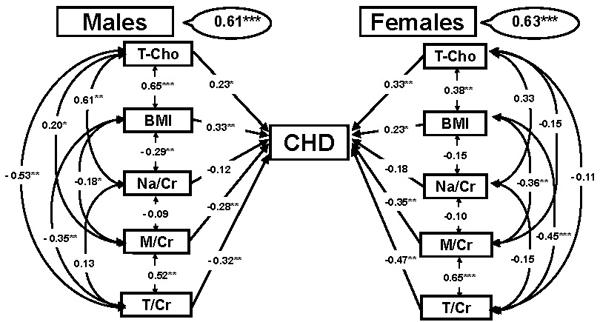
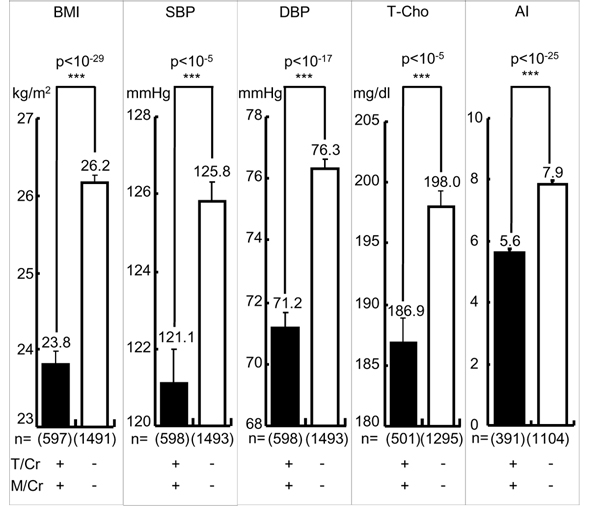
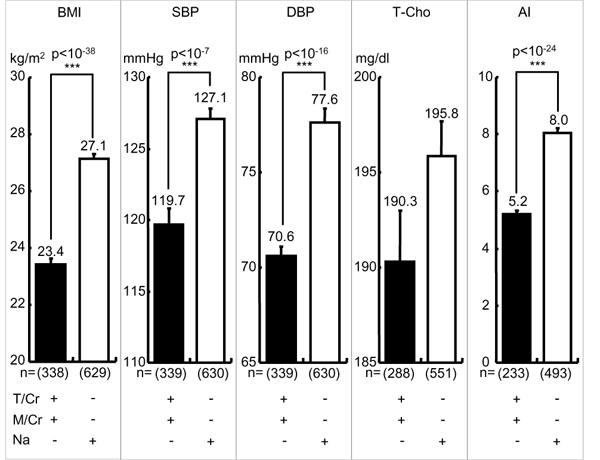
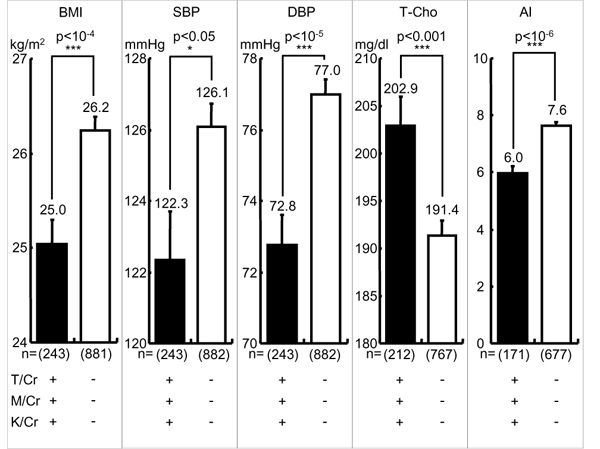
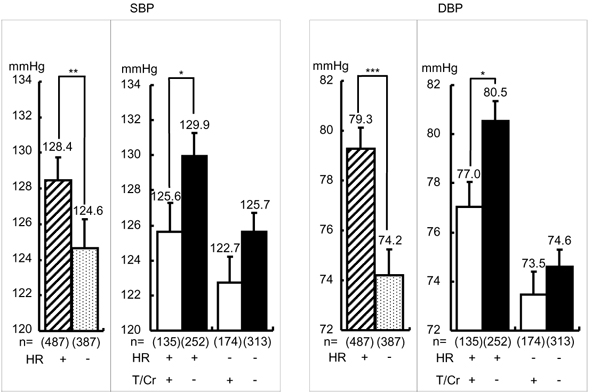
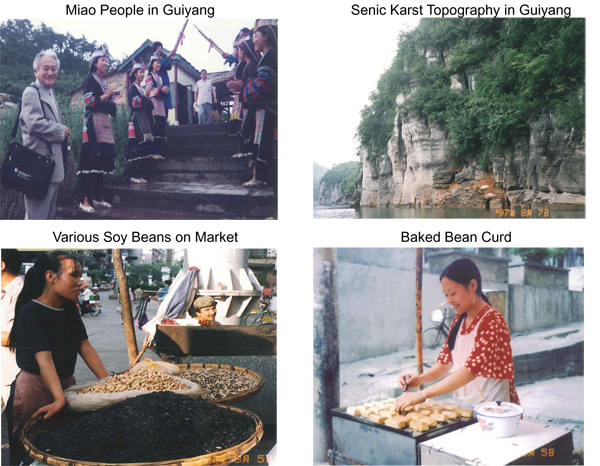
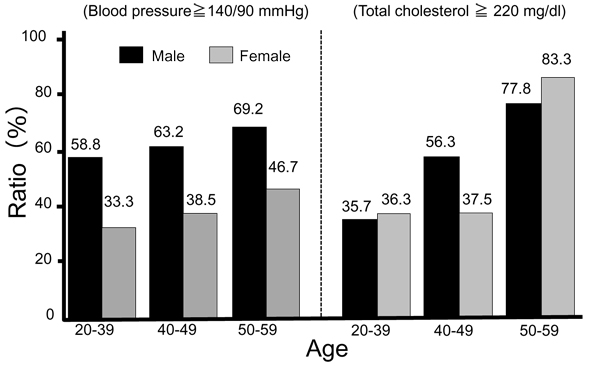
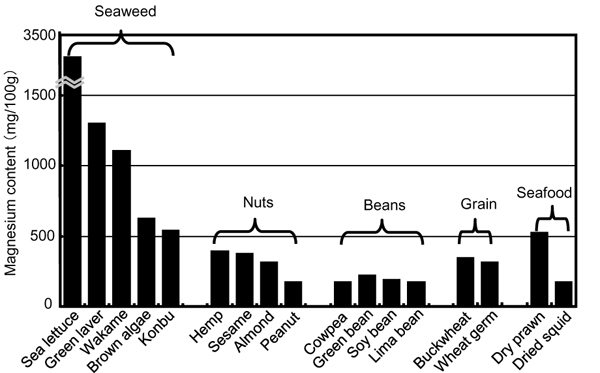
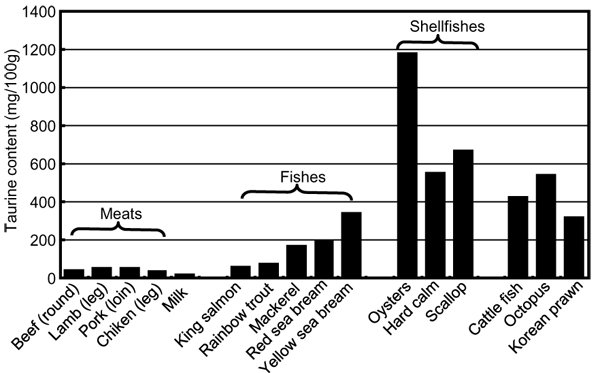
Taurine (T) was first noted as beneficial for stroke and cardiovascular diseases (CVD) prevention in genetic rat models, stroke-prone spontaneously hypertensive rats (SHRSP). The preventive mechanisms of T were ascribed to sympathetic modulation for reducing blood pressure (BP) and anti-inflammatory action. Recent epidemiological surveys revealed the involvement of inflammatory mediators in the pathogenesis of stroke and also atherosclerosis for which T was proven to be effective experimentally. Arterio-lipidosis prone rats, a substrain of SHRSP selectively bred for higher reactive hypercholesterolemia, quickly develop not only arterial fat deposition but also fatty liver which could be attenuated by dietary T supplementation. CARDIAC (CVD and Alimentary Comparison) Study was a WHO-coordinated multi-center epidemiological survey on diets and CVD risks and mortalities in 61 populations. Twenty-four-hour urinary (24U) T was inversely related significantly with coronary heart disease mortality. Higher 24U-T excreters had significantly lower body mass index, systolic and diastolic BP, total cholesterol (T-Cho), and atherogenic index (AI: T-Cho/high density lipoprotein-cholesterol) than lower T excreters. T effects on CVD risks were intensified in individuals whose 24U-T and -magnesium (M) excretions were higher. Furthermore, higher Na excreters with higher heart rate whose BP were significantly higher than those with lower heart rate were divided into two groups by the mean of 24U-T, high and low T excreters. Since the former showed significantly lower BP than the latter, T may beneficially affect salt-sensitive BP rise. Included among the typical 61 populations, were Guiyang, China or St. John's, Newfoundland, Canada where in which the means of both 24U-T and -M were high or low, respectively. The former and the latter had low and high CVD risks, respectively. Australian Aboriginals living at the coastal area in Victoria were supposed to eat T- and M-rich bush and sea foods and be free from CVD 200 years ago, but they presently have nearly the highest CVD risks indicating that T- and/or M-containing seafood, vegetables, fruits, nuts, milk, etc, similar to prehistoric hunters' and gatherers' food should be good for CVD prevention. The preventive effects of T, good for health and longevity, first noted experimentally, were also proven epidemiologically in humans.
Figures


Similar articles
-
Low cardiovascular risks in the middle aged males and females excreting greater 24-hour urinary taurine and magnesium in 41 WHO-CARDIAC study populations in the world.J Biomed Sci. 2010 Aug 24;17 Suppl 1(Suppl 1):S21. doi: 10.1186/1423-0127-17-S1-S21. J Biomed Sci. 2010. PMID: 20804596 Free PMC article.
-
Grading of Japanese Diet Intakes by 24-Hour Urine Analysis of Taurine and Soy Isoflavones in Relation to Cardiovascular Risks.Adv Exp Med Biol. 2022;1370:173-184. doi: 10.1007/978-3-030-93337-1_17. Adv Exp Med Biol. 2022. PMID: 35882793
-
Stroke-Prone SHR as Experimental Models for Cardiovascular Disease Risk Reduction in Humans.Biomedicines. 2022 Nov 18;10(11):2974. doi: 10.3390/biomedicines10112974. Biomedicines. 2022. PMID: 36428542 Free PMC article.
-
Gene-environment interaction in hypertension, stroke and atherosclerosis in experimental models and supportive findings from a world-wide cross-sectional epidemiological survey: a WHO-cardiac study.Clin Exp Pharmacol Physiol Suppl. 1992;20:43-52. Clin Exp Pharmacol Physiol Suppl. 1992. PMID: 1446409 Review.
-
Fish and lifestyle-related disease prevention: experimental and epidemiological evidence for anti-atherogenic potential of taurine.Clin Exp Pharmacol Physiol. 2004 Dec;31 Suppl 2:S20-3. doi: 10.1111/j.1440-1681.2004.04122.x. Clin Exp Pharmacol Physiol. 2004. PMID: 15649278 Review.
Cited by
-
Comparison of the Short-Term Effect of Coffee, Energy Drink, and Water on the Eyes in Young Healthy Subjects.Cureus. 2023 Nov 5;15(11):e48335. doi: 10.7759/cureus.48335. eCollection 2023 Nov. Cureus. 2023. PMID: 38060736 Free PMC article.
-
Taurine Supplementation Reduces Renal Nerve Activity in Male Rats in which Renal Nerve Activity was Increased by a High Sugar Diet.Adv Exp Med Biol. 2017;975 Pt 1:27-37. doi: 10.1007/978-94-024-1079-2_3. Adv Exp Med Biol. 2017. PMID: 28849441
-
Role of Mitochondria and Endoplasmic Reticulum in Taurine-Deficiency-Mediated Apoptosis.Nutrients. 2017 Jul 25;9(8):795. doi: 10.3390/nu9080795. Nutrients. 2017. PMID: 28757580 Free PMC article.
-
The evolving landscape of neurotoxicity by unconjugated bilirubin: role of glial cells and inflammation.Front Pharmacol. 2012 May 29;3:88. doi: 10.3389/fphar.2012.00088. eCollection 2012. Front Pharmacol. 2012. PMID: 22661946 Free PMC article.
-
Urinary Taurine Excretion and Risk of Late Graft Failure in Renal Transplant Recipients.Nutrients. 2019 Sep 13;11(9):2212. doi: 10.3390/nu11092212. Nutrients. 2019. PMID: 31540245 Free PMC article.
References
-
- Okamoto K, Aoki K. Development of a strain of spontaneously hypertensive rats. Jpn Circ J. 1963;27:282–293. - PubMed
-
- Yamori Y. In: Handbook of Hypertension. de Jong W. Amsterdam, editor. Elsevier; 1984. Development of the spontaneously hypertensive rat (SHR) and of various spontaneous rat models, and their implications. pp. 224–239.
-
- Okamoto T, Yamori Y, Nagaoka A. Establishment of the stroke-prone spontaneously hypertensive rat (SHR) Circ Res. 1974;34/35:143–153.
-
- Yamori Y. In: Handbook of Hypertension. de Jong W. Amsterdam, editor. Elsevier; 1984. The stroke-prone spontaneously hypertensive rat: Contribution to risk factor analysis and prevention of hypertensive diseases. pp. 240–255.
-
- WHO and WHO Collaborating Centers. CARDIAC (Cardiovascular Diseases and Alimentary Comparison) study protocol. Shimane/Geneva. 1986.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
