

Quantitative analysis of high-resolution computed tomography scans in severe asthma subphenotypes
- PMID: 20805170
- PMCID: PMC2975950
- DOI: 10.1136/thx.2010.136374
Quantitative analysis of high-resolution computed tomography scans in severe asthma subphenotypes
Abstract
Background: Severe asthma is a heterogeneous condition. Airway remodelling is a feature of severe asthma and can be determined by the assessment of high-resolution computed tomography (HRCT) scans. The aim of this study was to assess whether airway remodelling is restricted to specific subphenotypes of severe asthma.
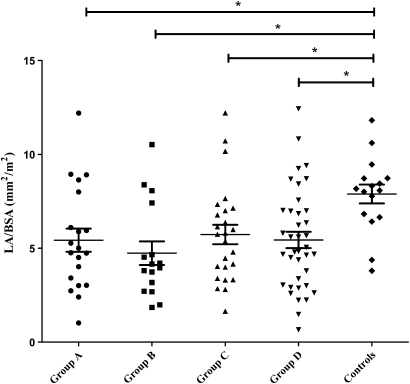
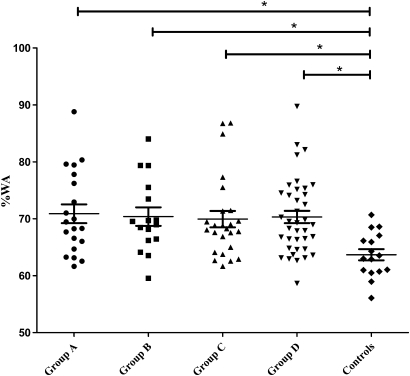
Methods: A retrospective analysis was performed of HRCT scans from subjects who had attended a single-centre severe asthma clinic between 2003 and 2008. The right upper lobe apical segmental bronchus (RB1) dimensions were measured and the clinical and sputum inflammatory characteristics associated with RB1 geometry were assessed by univariate and multivariate regression analyses. Longitudinal sputum data were available and were described as area under the time curve (AUC). Comparisons were made in RB1 geometry across subjects in four subphenotypes determined by cluster analysis, smokers and non-smokers, and subjects with and without persistent airflow obstruction.
Results: Ninety-nine subjects with severe asthma and 16 healthy controls were recruited. In the subjects with severe asthma the RB1 percentage wall area (%WA) was increased (p=0.009) and lumen area (LA)/body surface area (BSA) was decreased (p=0.008) compared with controls but was not different across the four subphenotypes. Airway geometry was not different between smokers and non-smokers and RB1 %WA was increased in those with persistent airflow obstruction. RB1 %WA in severe asthma was best associated with airflow limitation and persistent neutrophilic airway inflammation (model R(2)=0.27, p=0.001).
Conclusions: Airway remodelling of proximal airways occurs in severe asthma and is associated with impaired lung function and neutrophilic airway inflammation.
Conflict of interest statement
Figures


References
-
- Wenzel S. Severe asthma in adults. Am J Respir Crit Care Med 2005;172:149–60 - PubMed
-
- Antonicelli L, Bucca C, Neri M, et al. Asthma severity and medical resource utilisation. Eur Respir J 2004;23:723–9 - PubMed
-
- Holgate ST. Epithelium dysfunction in asthma. J Allergy Clin Immunol 2007;120:1233–46 - PubMed
-
- Niimi A, Matsumoto H, Amitani R, et al. Airway wall thickness in asthma assessed by computed tomography: relation to clinical indices. Am J Respir Crit Care Med 2000;162:1518–23 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous