

Histology atlas of the developing mouse hepatobiliary system with emphasis on embryonic days 9.5-18.5
- PMID: 20805319
- PMCID: PMC3490618
- DOI: 10.1177/0192623310374329
Histology atlas of the developing mouse hepatobiliary system with emphasis on embryonic days 9.5-18.5
Abstract
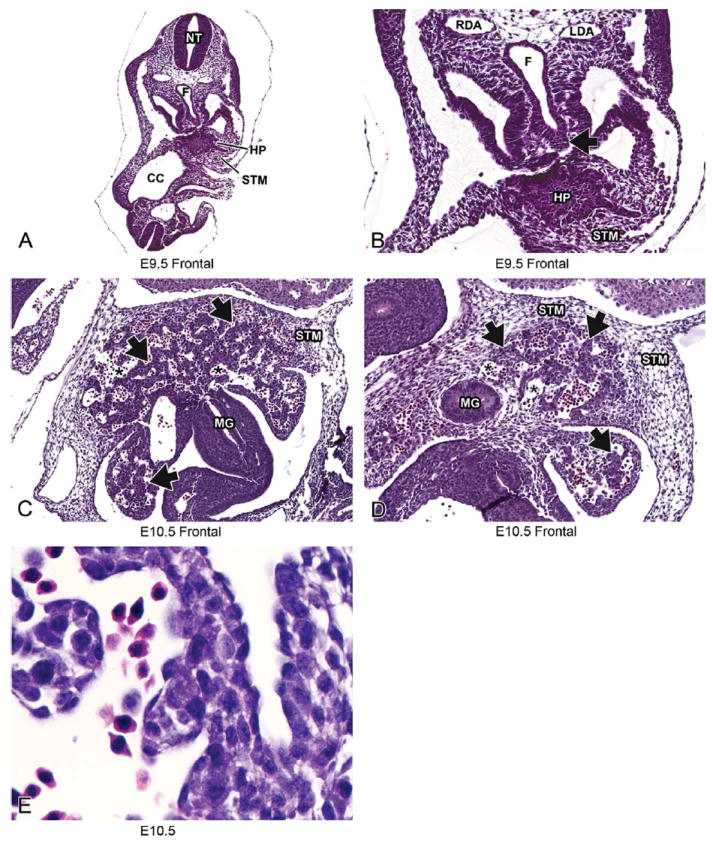
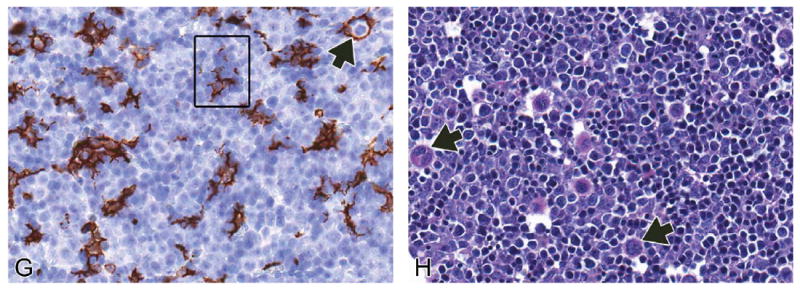
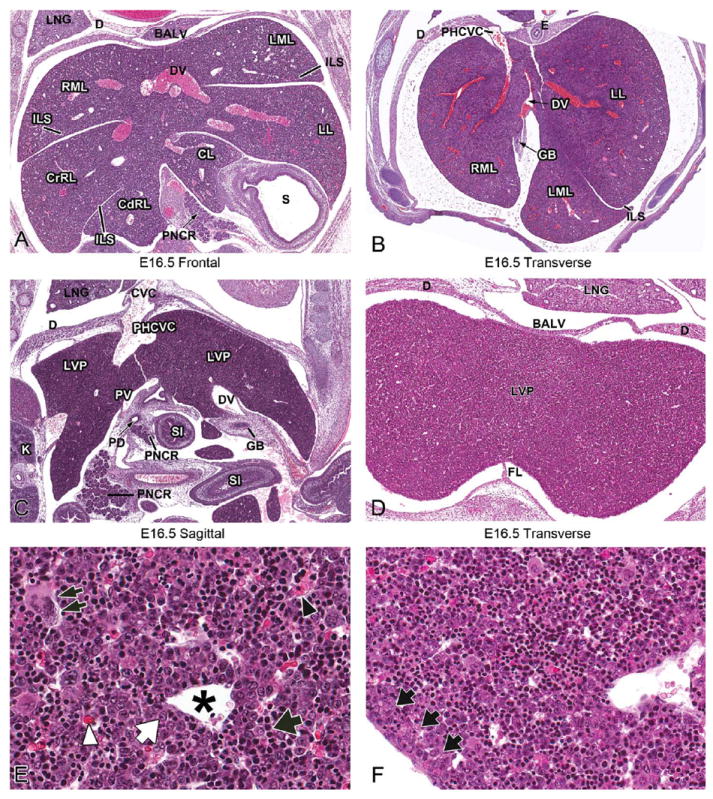
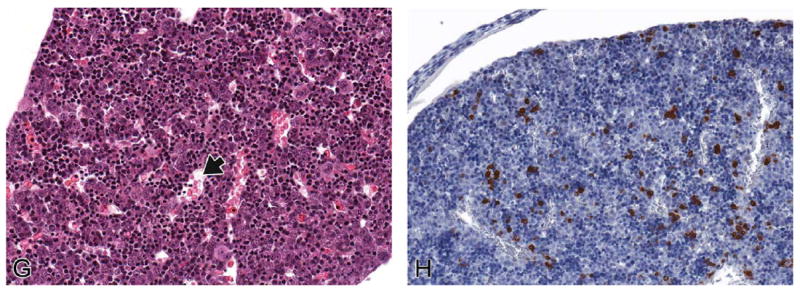
Animal model phenotyping, in utero exposure toxicity studies, and investigation into causes of embryonic, fetal, or perinatal deaths have required pathologists to recognize and diagnose developmental disorders in spontaneous and engineered mouse models of disease. In mammals, the liver is the main site of hematopoiesis during fetal development, has endocrine and exocrine functions important for maintaining homeostasis in fetal and adult life; and performs other functions including waste detoxification, production and removal of glucose, glycogen storage, triglyceride and fatty acid processing, and serum protein production. Due to its role in many critical functions, alterations in the size, morphology, or function(s) of the liver often lead to embryonic lethality. Many publications and websites describe individual aspects of hepatobiliary development at defined stages. However, no single resource provides a detailed histological evaluation of H&E-stained sections of the developing murine liver and biliary systems using high-magnification and high-resolution color images. The work herein provides a histology atlas of hepatobiliary development between embryonic days 9.5-18.5. Although the focus of this work is normal hepatobiliary development, common defects in liver development are also described as a reference for pathologists who may be asked to phenotype mice with congenital, inherited, or treatment-related hepatobiliary defects. Authors' note: All digital images can be viewed online at https://niehsimagesepl-inc.com with the username "ToxPathLiver" and the password "embryolivers."
Figures










Similar articles
-
Histology atlas of the developing mouse heart with emphasis on E11.5 to E18.5.Toxicol Pathol. 2009 Jun;37(4):395-414. doi: 10.1177/0192623309335060. Epub 2009 Apr 9. Toxicol Pathol. 2009. PMID: 19359541 Free PMC article. Review.
-
Histology Atlas of the Developing Mouse Hepatobiliary Hemolymphatic Vascular System with Emphasis on Embryonic Days 11.5-18.5 and Early Postnatal Development.Toxicol Pathol. 2016 Jul;44(5):705-25. doi: 10.1177/0192623316630836. Epub 2016 Mar 8. Toxicol Pathol. 2016. PMID: 26961180 Free PMC article.
-
Histology Atlas of the Developing Prenatal and Postnatal Mouse Central Nervous System, with Emphasis on Prenatal Days E7.5 to E18.5.Toxicol Pathol. 2017 Aug;45(6):705-744. doi: 10.1177/0192623317728134. Epub 2017 Sep 11. Toxicol Pathol. 2017. PMID: 28891434 Free PMC article.
-
Excretion of biliary compounds during intrauterine life.World J Gastroenterol. 2009 Feb 21;15(7):817-28. doi: 10.3748/wjg.15.817. World J Gastroenterol. 2009. PMID: 19230042 Free PMC article. Review.
-
Estrogen Acts Through Estrogen Receptor 2b to Regulate Hepatobiliary Fate During Vertebrate Development.Hepatology. 2020 Nov;72(5):1786-1799. doi: 10.1002/hep.31184. Hepatology. 2020. PMID: 32060934 Free PMC article.
Cited by
-
Volumetric imaging reveals VEGF-C-dependent formation of hepatic lymph vessels in mice.Front Cell Dev Biol. 2022 Aug 16;10:949896. doi: 10.3389/fcell.2022.949896. eCollection 2022. Front Cell Dev Biol. 2022. PMID: 36051444 Free PMC article.
-
Concomitant genetic defects potentiate the adverse impact of prenatal alcohol exposure on cardiac outflow tract maturation.Birth Defects Res. 2022 Feb;114(3-4):105-115. doi: 10.1002/bdr2.1968. Epub 2021 Dec 3. Birth Defects Res. 2022. PMID: 34859965 Free PMC article.
-
Spatiotemporal dynamics of fetal liver hematopoietic niches.J Exp Med. 2025 Feb 3;222(2):e20240592. doi: 10.1084/jem.20240592. Epub 2025 Jan 7. J Exp Med. 2025. PMID: 39775824 Free PMC article.
-
Mouse extraembryonic arterial vessels harbor precursors capable of maturing into definitive HSCs.Blood. 2013 Oct 3;122(14):2338-45. doi: 10.1182/blood-2012-12-470971. Epub 2013 Jul 17. Blood. 2013. PMID: 23863896 Free PMC article.
-
Proceedings of the 2016 National Toxicology Program Satellite Symposium.Toxicol Pathol. 2017 Jan;45(1):11-51. doi: 10.1177/0192623316672074. Epub 2016 Nov 11. Toxicol Pathol. 2017. PMID: 27821709 Free PMC article.
References
-
- Apte U, Zeng G, Thompson MD, Muller P, Micsenyi A, Cieply B, Kaestner KH, Monga SP. Beta-Catenin is critical for early postnatal liver growth. Am J Physiol Gastrointest Liver Physiol. 2007;292:G1578–85. - PubMed
-
- Asano H, Kobayashi M, Hoshino T. The hemopoietic microenvironment in the fetal liver of mice: relationship between developing hepatocytes and erythroblasts. J Electron Microsc (Tokyo) 1987;36:15–25. - PubMed
-
- Chasis JA. Erythroblastic islands: Specialized microenvironmental niches for erythropoiesis. Curr Opin Hematol. 2006;13:137–41. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
