

Nonconvulsive seizures after traumatic brain injury are associated with hippocampal atrophy
- PMID: 20805525
- PMCID: PMC2938965
- DOI: 10.1212/WNL.0b013e3181f07334
Nonconvulsive seizures after traumatic brain injury are associated with hippocampal atrophy
Abstract
Objective: To determine if posttraumatic nonconvulsive electrographic seizures result in long-term brain atrophy.
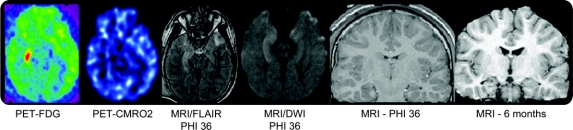
Methods: Prospective continuous EEG (cEEG) monitoring was done in 140 patients with moderate to severe traumatic brain injury (TBI) and in-depth study of 16 selected patients was done using serial volumetric MRI acutely and at 6 months after TBI. Fluorodeoxyglucose PET was done in the acute stage in 14/16 patients. These data were retrospectively analyzed after collection of data for 7 years.
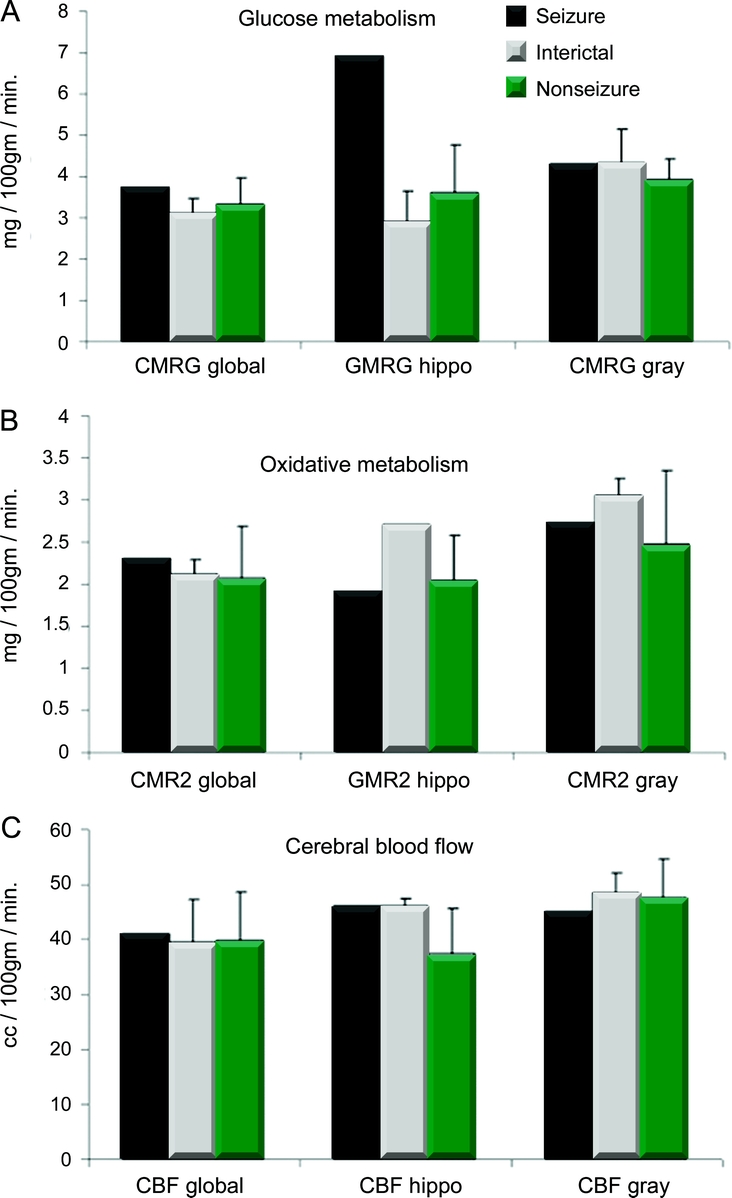
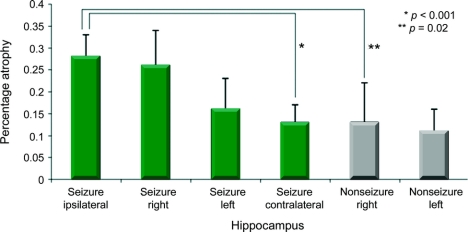
Results: cEEG detected seizures in 32/140 (23%) of the entire cohort. In the selected imaging subgroup, 6 patients with seizures were compared with a cohort of 10 age- and GCS-matched patients with TBI without seizures. In this subgroup, the seizures were repetitive and constituted status epilepticus in 4/6 patients. Patients with seizures had greater hippocampal atrophy as compared to those without seizures (21 +/- 9 vs 12 +/- 6%, p = 0.017). Hippocampi ipsilateral to the electrographic seizure focus demonstrated a greater degree of volumetric atrophy as compared with nonseizure hippocampi (28 +/- 5 vs 13 +/- 9%, p = 0.007). A single patient had an ictal PET scan which demonstrated increased hippocampal glucose uptake.
Conclusion: Acute posttraumatic nonconvulsive seizures occur frequently after TBI and, in a selected subgroup, appear to be associated with disproportionate long-term hippocampal atrophy. These data suggest anatomic damage is potentially elicited by nonconvulsive seizures in the acute postinjury setting.
Figures
Comment in
-
Nonconvulsive status epilepticus and brain damage: further evidence, more questions.Neurology. 2010 Aug 31;75(9):760-1. doi: 10.1212/WNL.0b013e3181f32141. Neurology. 2010. PMID: 20805520 No abstract available.
References
-
- Vincent JL, Berre J. Primer on medical management of severe brain injury. Crit Care Med 2005;33:1392–1399. - PubMed
-
- Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology 2004;62:1743–1748. - PubMed
-
- Vespa P, O'Phelan K, Mirabelli J, et al. Acute seizures after intracerebral hemorrhage: A factor in progressive midline shift and outcome. Neurology 2003;60:1441–1446. - PubMed
-
- Bergsneider MA, Hovda DA, Shalmon E, et al. Cerebral hyperglycolysis following severe human traumatic brain injury: a positron emission tomography study. J Neurosurg 1997;86:241–251. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 EY15311/EY/NEI NIH HHS/United States
- P50 HL60296/HL/NHLBI NIH HHS/United States
- R01 NS036524/NS/NINDS NIH HHS/United States
- NS 049471/NS/NINDS NIH HHS/United States
- 1R21NS057252-01A1/NS/NINDS NIH HHS/United States
- 1 R01 NS055910-01A1/NS/NINDS NIH HHS/United States
- R01 NS 049471/NS/NINDS NIH HHS/United States
- R01 NS051591/RG3915/NS/NINDS NIH HHS/United States
- R01NS 49471/NS/NINDS NIH HHS/United States
- P50 NS044378/NS/NINDS NIH HHS/United States
- 1 R01 NS052406/NS/NINDS NIH HHS/United States
- R21 MH075658/MH/NIMH NIH HHS/United States
- 1 R21 NS057252-01A1/NS/NINDS NIH HHS/United States
- 1 P01 NS058489-01/NS/NINDS NIH HHS/United States
- 1 R01NS27544/NS/NINDS NIH HHS/United States
- R01 EB00822/EB/NIBIB NIH HHS/United States
- NS 02089/NS/NINDS NIH HHS/United States
- R01 NS049471/NS/NINDS NIH HHS/United States
- R01 NR009116/NR/NINR NIH HHS/United States
- R01NS46018/NS/NINDS NIH HHS/United States
- R01MH081864/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical