

Electroconvulsive therapy stimulus parameters: rethinking dosage
- PMID: 20805726
- PMCID: PMC2933093
- DOI: 10.1097/YCT.0b013e3181e48165
Electroconvulsive therapy stimulus parameters: rethinking dosage
Abstract
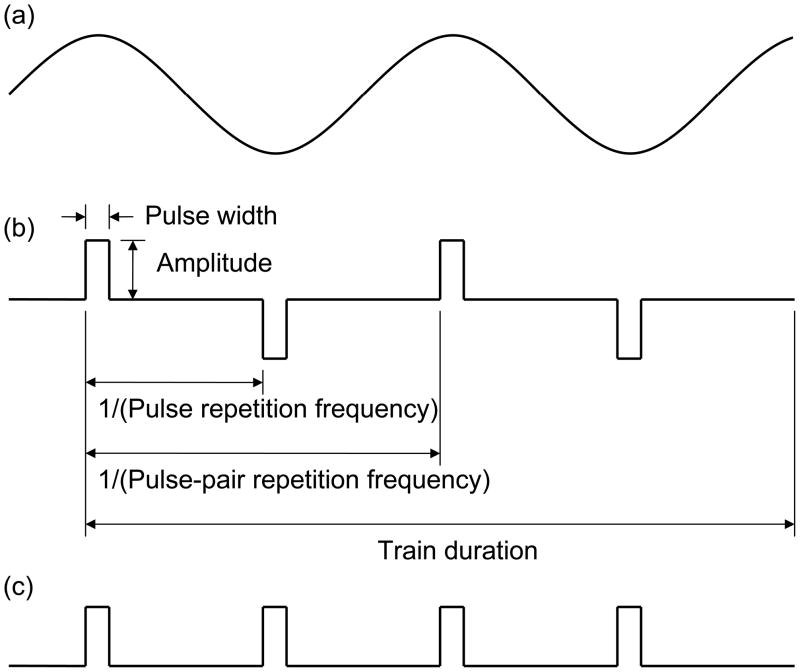
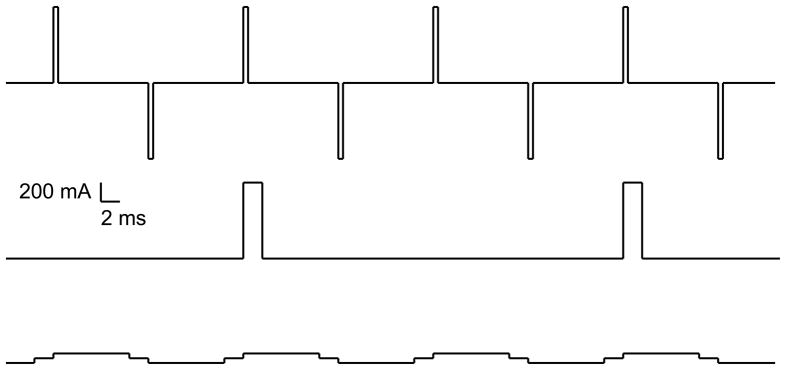
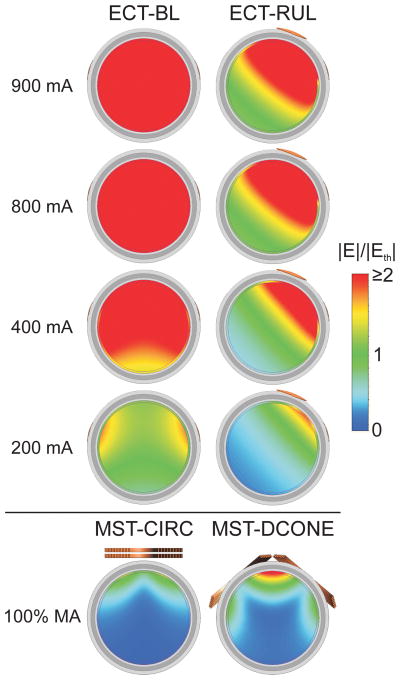
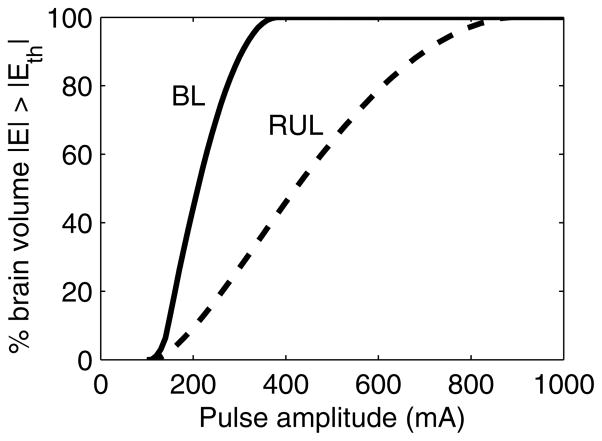
In this article, we review the parameters that define the electroconvulsive therapy (ECT) electrical stimulus and discuss their biophysical roles. We also present the summary metrics of charge and energy that are conventionally used to describe the dose of ECT and the rules commonly deployed to individualize the dose for each patient. We then highlight the limitations of these summary metrics and dosing rules in that they do not adequately capture the roles of the distinct stimulus parameters. Specifically, there is strong theoretical and empirical evidence that stimulus parameters (pulse amplitude, shape, and width, and train frequency, directionality, polarity, and duration) exert unique neurobiological effects that are important for understanding ECT outcomes. Consideration of the distinct stimulus parameters, in conjunction with electrode placement, is central to further optimization of ECT dosing paradigms to improve the risk-benefit ratio. Indeed, manipulation of specific parameters, such as reduction of pulse width and increase in number of pulses, has already resulted in dramatic reduction of adverse effects, while maintaining efficacy. Furthermore, the manipulation of other parameters, such as current amplitude, which are commonly held at fixed, high values, might be productively examined as additional means of targeting and individualizing the stimulus, potentially reducing adverse effects. We recommend that ECT dose be defined using all stimulus parameters rather than a summary metric. All stimulus parameters should be noted in treatment records and published reports. To enable research on optimization of dosing paradigms, we suggest that ECT devices provide capabilities to adjust and display all stimulus parameters.
Figures
References
-
- Kalinowsky LB, Hippius H. Pharmacological, convulsive, and other somatic treatments in psychiatry. New York: Grune & Stratton; 1969.
-
- Kalinowsky LB. ECT instrumentation. Biol Psychiatry. 1988;24:361–362. - PubMed
-
- Weiner RD, Rogers HJ, Davidson JR, et al. Effects of stimulus parameters on cognitive side effects. Ann N Y Acad Sci. 1986;462:315–325. - PubMed
-
- Sackeim HA, Prudic J, Devanand DP, et al. A prospective, randomized, double-blind comparison of bilateral and right unilateral electroconvulsive therapy at different stimulus intensities. Arch Gen Psychiatry. 2000;57:425–434. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
