

Extreme stress hyperglycemia during acute illness in a pediatric emergency department
- PMID: 20805780
- PMCID: PMC4381194
- DOI: 10.1097/PEC.0b013e3181ef0488
Extreme stress hyperglycemia during acute illness in a pediatric emergency department
Abstract
Objectives: Although mild stress hyperglycemia in pediatric illness is common, severe hyperglycemic responses (≥300 mg/dL [16.7 mmol/L]) to stress are unusual. We sought to determine the incidence and course of extreme stress hyperglycemia (ESH) in acute pediatric illness, including whether it is a marker of increased mortality or associated with subsequent development of diabetes mellitus (DM).
Methods: We retrospectively reviewed a cohort of 55,120 consecutive visits over 6 years to a pediatric emergency department at which blood glucose concentrations were measured and report on visits with laboratory glucose 300 mg/dL (16.7 mmol/L) or greater without DM.
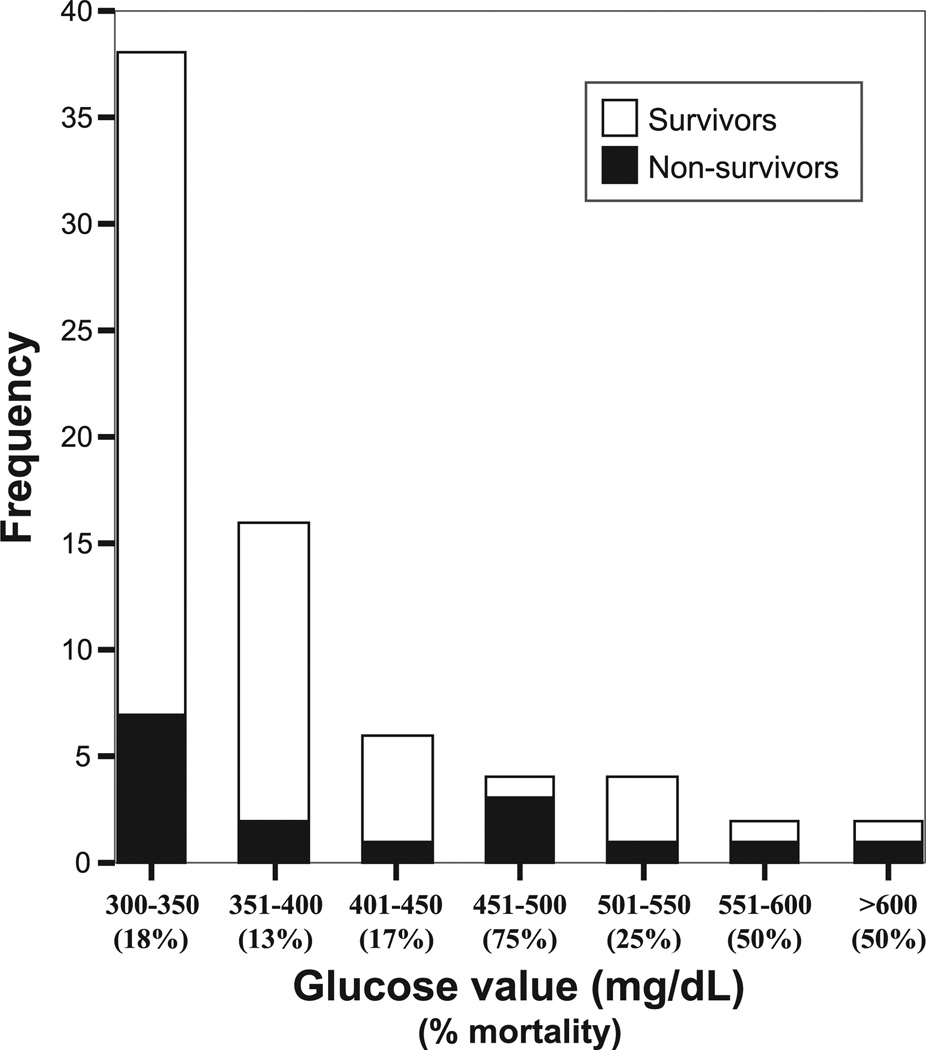
Results: There were 72 cases of ESH (incidence of 0.13%). Median age was 8.8 years; 63% were male. The most common diagnoses were respiratory illness (49%), trauma (15%), and seizure (8%), and 65% of patients had received glucose-influencing interventions before evaluation. Eighty-five percent were ill appearing, 60% were admitted to the intensive care unit, and half had acidemic pH values. The overall mortality rate was 22%. Despite treatment of hyperglycemia in only 8 patients, glucose concentrations decreased to 150 mg/dL (8.3 mmol/L) or less within 48 hours in 67% and before discharge or death in 85% of patients. Preceding symptoms and concurrent laboratory results were helpful to exclude diabetes, and none of the surviving patients with follow-up available went on to develop type 1 or 2 DM.
Conclusions: Although rare, ESH (≥300 mg/dL [16.7 mmol/L]) does occur in acute pediatric illness, in most cases is at least partially iatrogenic, and is a marker of severe illness and high mortality. Normoglycemia is typically restored quickly with treatment of the primary illness. No association was found with a subsequent diagnosis of DM.
Figures
Comment in
-
Glucose metabolism disturbances in acute pediatric illness.Pediatr Emerg Care. 2011 May;27(5):452-4. doi: 10.1097/PEC.0b013e31821c987b. Pediatr Emerg Care. 2011. PMID: 21546818 No abstract available.
References
-
- Marik PE, Raghavan M. Stress-hyperglycemia, insulin and immunomodulation in sepsis. Intensive Care Med. 2004;30:748–756. - PubMed
-
- Chernow B, Rainey T, Heller R, et al. Marked stress hyperglycemia in a child. Crit Care Med. 1982;10:696–697. - PubMed
-
- Rayfield EJ, Curnow RT, George DT, et al. Impaired carbohydrate metabolism during a mild viral illness. N Engl J Med. 1973;289:618–620. - PubMed
-
- Rocha DM, Santeusanio F, Faloona GR, et al. Abnormal pancreatic alpha-cell function in bacterial infections. N Engl J Med. 1973;288:700–703. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
