

Very-Low-Dose Pegylated Interferon a2a Plus Ribavirin Therapy for Advanced Liver Cirrhosis Type C: A Possible Therapeutic Alternative without Splenic Intervention
- PMID: 20805953
- PMCID: PMC2929425
- DOI: 10.1159/000318742
Very-Low-Dose Pegylated Interferon a2a Plus Ribavirin Therapy for Advanced Liver Cirrhosis Type C: A Possible Therapeutic Alternative without Splenic Intervention
Abstract
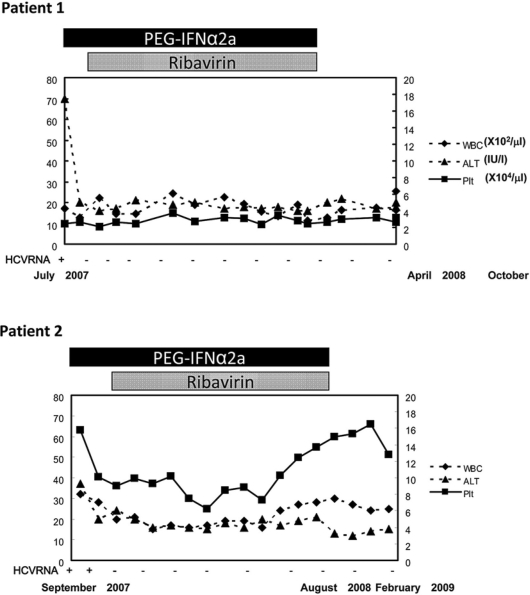
Despite the recent progress in interferon (IFN) therapies for chronic hepatitis C, liver cirrhosis remains refractory. One of the major obstacles to successful IFN therapy is low platelet count. Currently, splenic interventions, such as partial splenic embolization (PSE) or surgical splenectomy, have been applied effectively and make standard IFN therapy possible. However, there may be a group of patients with low platelet counts who can be treated without splenic intervention. We here report two patients with advanced type C liver cirrhosis who were successfully treated using very-low-dose pegylated interferon a2a plus ribavirin. One patient had a very low platelet count (2.5 x 10(4)/mul) due to splenomegaly before treatment. However, pretreatment serum HCV titers were low in both patients and early viral responses were obtained in both. Because PSE or splenectomy may still have some safety concerns, this attenuated IFN treatment protocol can be an alternative therapeutic option for patients with advanced type C liver disease, but good virological factors for sustained virological response.
Figures
Similar articles
-
Safe use of pegylated interferon/ribavirin in hepatitis C virus cirrhotic patients with hypersplenism after partial splenic embolization.Eur J Gastroenterol Hepatol. 2005 Nov;17(11):1157-64. doi: 10.1097/00042737-200511000-00002. Eur J Gastroenterol Hepatol. 2005. PMID: 16215426
-
Combination therapy of low-dose of PegIFNa-2a and ribavirin for patients with HCV-infected decompensated cirrhosis.Hepatogastroenterology. 2013 Sep;60(126):1391-8. doi: 10.5754/hge121194. Hepatogastroenterology. 2013. PMID: 23635509
-
Safety and efficacy of partial splenic embolization in telaprevir-based triple therapy for chronic hepatitis C.Intern Med. 2015;54(2):119-26. doi: 10.2169/internalmedicine.54.3066. Epub 2015 Jan 15. Intern Med. 2015. PMID: 25743001
-
Interferon-alpha-2b plus ribavirin: a review of its use in the management of chronic hepatitis C.Drugs. 2002;62(3):507-56. doi: 10.2165/00003495-200262030-00009. Drugs. 2002. PMID: 11827565 Review.
-
Consensus guidelines for the management of hepatitis C infection.Saudi Med J. 2003 Jul;24 Suppl 2:S99-118. Saudi Med J. 2003. PMID: 25121186
References
-
- NIH Consensus Statement on Management of Hepatitis C 2002 NIH Consens State Sci Statements. 2002;19:1–46. - PubMed
-
- Hayashi N, Takehara T. Antiviral therapy for chronic hepatitis C: past, present, and future. J Gastroenterol. 2006;41:17–27. - PubMed
-
- Zeuzem S. Interferon-based therapy for chronic hepatitis C: current and future perspectives. Nat Clin Pract Gastroenterol Hepatol. 2008;5:610–622. - PubMed
-
- Heathcote EJ. Antiviral therapy: chronic hepatitis C. J Viral Hepat. 2007;14(suppl 1):82–88. - PubMed
-
- Everson GT, Hoefs JC, Seeff LB, et al. Impact of disease severity on outcome of antiviral therapy for chronic hepatitis C: Lessons from the HALT-C trial. Hepatology. 2006;44:1675–1684. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
