

Changing epidemiology of serious bacterial infections in febrile infants without localizing signs
- PMID: 20805983
- PMCID: PMC2929196
- DOI: 10.1371/journal.pone.0012448
Changing epidemiology of serious bacterial infections in febrile infants without localizing signs
Abstract
Objective: Historically, management of infants with fever without localizing signs (FWLS) has generated much controversy, with attempts to risk stratify based on several criteria. Advances in medical practice may have altered the epidemiology of serious bacterial infections (SBIs) in this population. We conducted this study to test the hypothesis that the rate of SBIs in this patient population has changed over time.
Patients and methods: We performed a retrospective review of all infants meeting FWLS criteria at our institution from 1997-2006. We examined all clinical and outcome data and performed statistical analysis of SBI rates and ampicillin resistance rates.
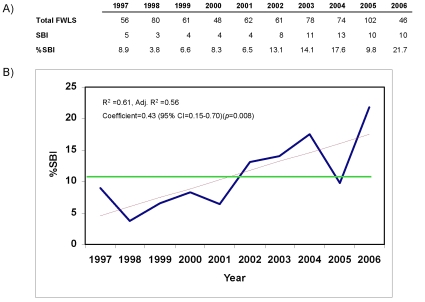
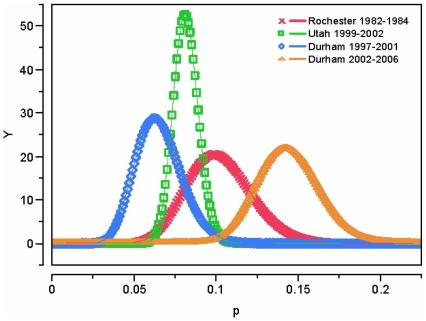
Results: 668 infants met criteria for FWLS. The overall rate of SBIs was 10.8%, with a significant increase from 2002-2006 (52/361, 14.4%) compared to 1997-2001 (20/307, 6.5%) (p = 0.001). This increase was driven by an increase in E. coli urinary tract infections (UTI), particularly in older infants (31-90 days).
Conclusions: We observed a significant increase in E. coli UTI among FWLS infants with high rates of ampicillin resistance. The reasons are likely to be multifactorial, but the results themselves emphasize the need to examine urine in all febrile infants <90 days and consider local resistance patterns when choosing empiric antibiotics.
Conflict of interest statement
Figures
References
-
- Crain EF, Shelov SP. Febrile infants: predictors of bacteremia. J Pediatr. 1982;101:686–689. - PubMed
-
- Roberts KB, Charney E, Sweren RJ, Ahonkhai VI, Bergman DA, et al. Urinary tract infection in infants with unexplained fever: a collaborative study. J Pediatr. 1983;103:864–867. - PubMed
-
- Marshall R, Teele DW, Klein JO. Unsuspected bacteremia due to Haemophilus influenzae: outcome in children not initially admitted to hospital. J Pediatr. 1979;95:690–695. - PubMed
-
- McGowan JE, Jr, Bratton L, Klein JO, Finland M. Bacteremia in febrile children seen in a “walk-in” pediatric clinic. N Engl J Med. 1973;288:1309–1312. - PubMed
-
- Dagan R, Powell KR, Hall CB, Menegus MA. Identification of infants unlikely to have serious bacterial infection although hospitalized for suspected sepsis. J Pediatr. 1985;107:855–860. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
