

Review
Acute lung injury and the acute respiratory distress syndrome: pathophysiology and treatment
Affiliations
- PMID: 20806836
- PMCID: PMC6188356
Item in Clipboard
Review
Acute lung injury and the acute respiratory distress syndrome: pathophysiology and treatment
Mo Med.
2010 Jul-Aug.
Abstract
Acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) represent a spectrum of acute respiratory failure with diffuse, bilateral lung injury and severe hypoxemia caused by non-cardiogenic pulmonary edema. Failure may be initiated by pulmonary or extrapulmonary insults (e.g., pneumonia, sepsis, trauma, aspiration) that increase alveolar epithelial endothelial permeability, flood alveoli, and reduce lung compliance. The only treatment proven to improve survival is mechanical ventilation using a 'lung protective strategy' with tidal volume =6 mL/kg predicted body weight. Although mortality can exceed 50%, survivors have a good prognosis for recovery of lung function.
Figures
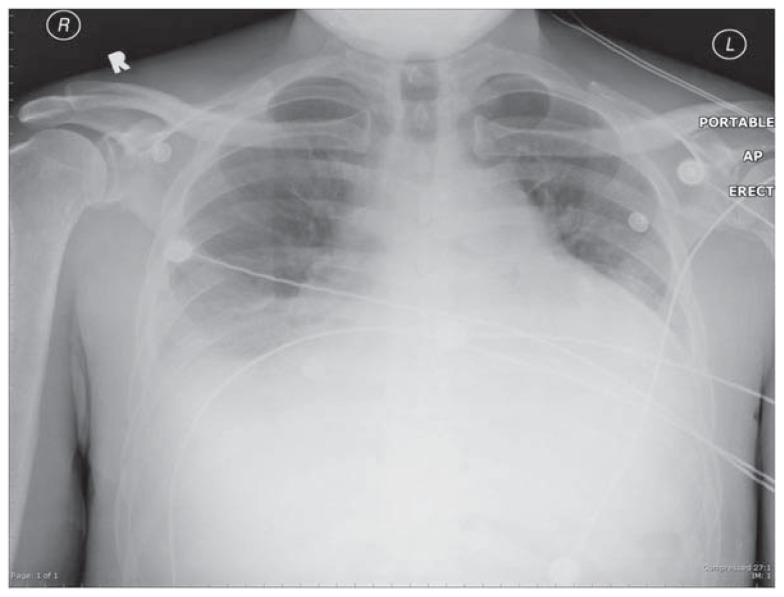
Chest radiograph showing cardiomegaly and bilateral pleural effusions. Such findings are compatible with elevated left atrial pressure, interstitial cardiogenic pulmonary edema, and LV systolic dysfunction as are seen in congestive heart failure.
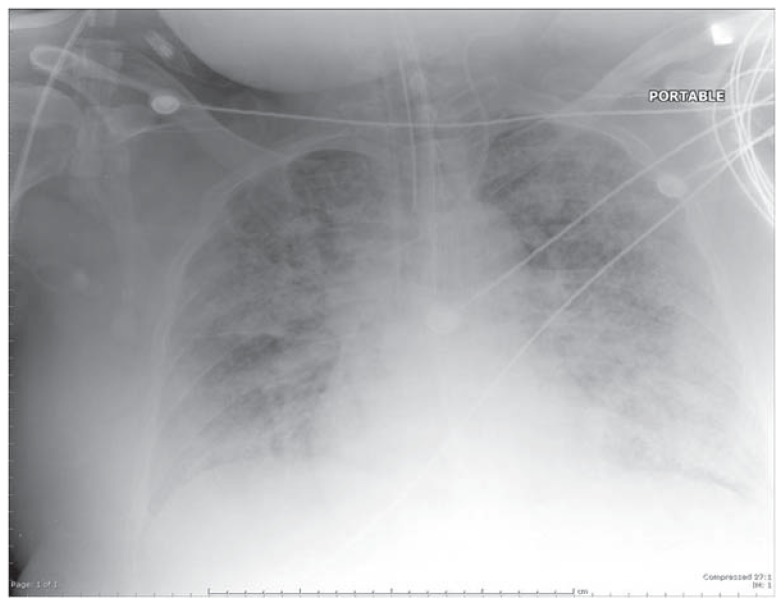
Chest radiograph showing diffuse, bilateral pulmonary infiltrates in all lung quadrants (acute air-space disease) typical of ALI/ARDS. The costophrenic angles are relatively clear, indicating absence of pleural effusions.
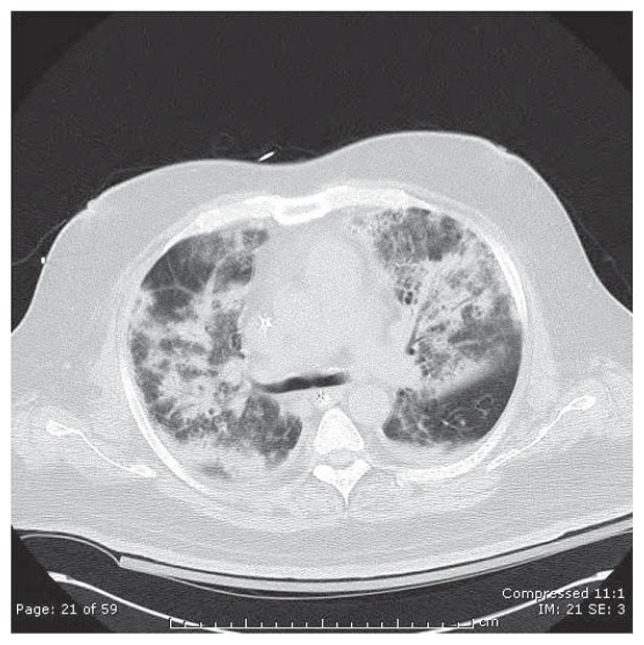
Computed tomographic (CT) scan of the chest (lung attenuation window) in a patient with severe ARDS due to bilateral S. pneumoniae pneumonia. Note extensive opacification of alveolar units & prominent air bronchograms, compared with the small residual area of normal, radiolucent (black)-appearing lung in the right upper and left lower portions of this image.
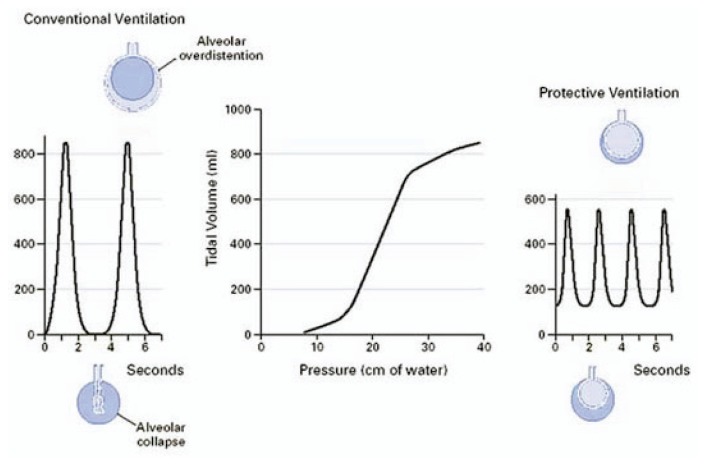
Effects on achieved tidal volumes in sedated patients using conventional mechanical ventilation (left) or when using a protective lung ventilation strategy (right). From Tobin MJ. © 2001, Massachusetts Medical Society. All rights reserved.
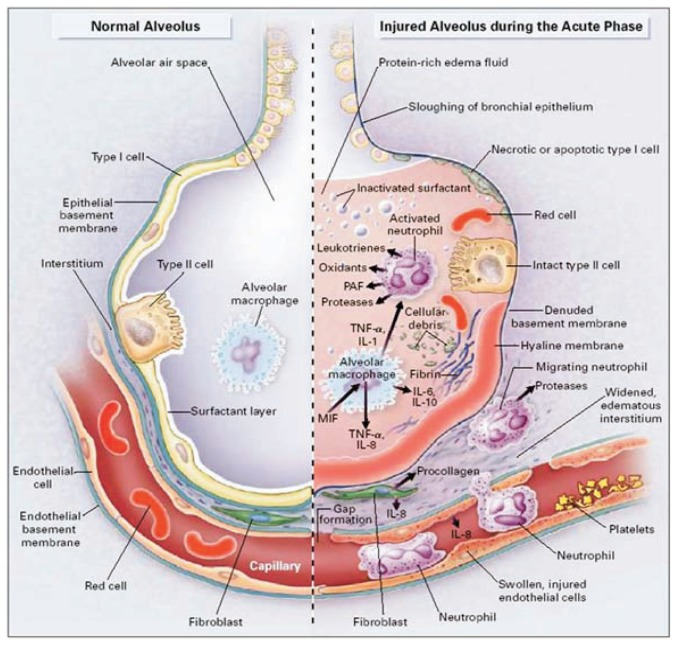
The normal alveolus vs. the acutely injured alveolus in ALI/ARDS. From: Ware LB and Matthay M. © 2000, Massachusetts Medical Society. All rights reserved.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Looney MR, Gropper MA, Matthay MA. Transfusion-related lung injury. Chest. 2004;126:249–258. - PubMed
-
- Rubenfeld GD, Herridge MS. Epidemiology and outcomes of acute lung injury. Chest. 2007;131:554–562. - PubMed
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS: Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149:818–824. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources