

Characterizing abdominal pain in IBS: guidance for study inclusion criteria, outcome measurement and clinical practice
- PMID: 20807217
- PMCID: PMC4118306
- DOI: 10.1111/j.1365-2036.2010.04443.x
Characterizing abdominal pain in IBS: guidance for study inclusion criteria, outcome measurement and clinical practice
Abstract
Background: Although irritable bowel syndrome (IBS) is a multisymptom disorder, abdominal pain drives illness severity more than other symptoms. Despite consensus that IBS trials should measure pain to define study entry and determine efficacy, the optimal method of measuring pain remains uncertain.
Aim: To determine whether combining information from multiple pain dimensions may capture the IBS illness experience more effectively than the approach of measuring 'pain predominance' or pain intensity alone.
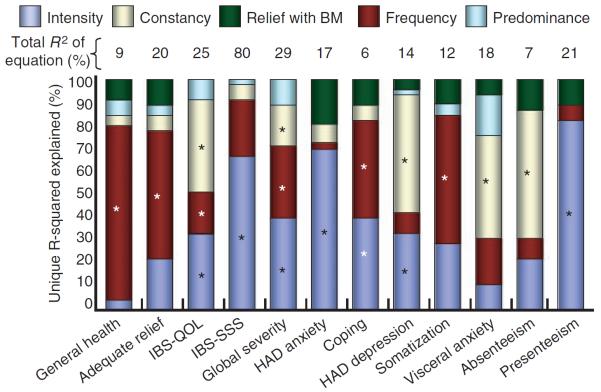
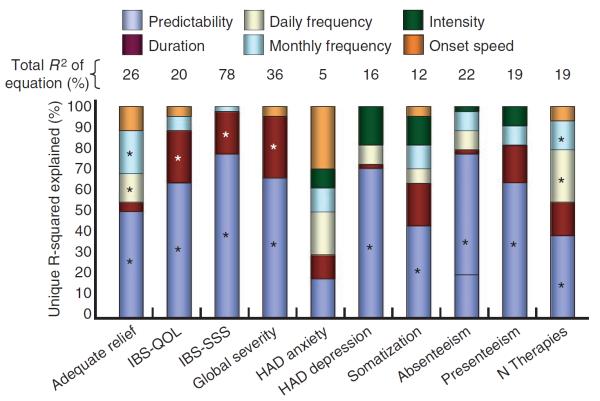
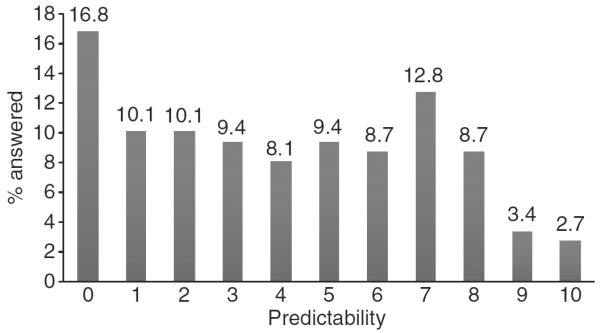
Methods: Irritable bowel syndrome patients rated dimensions of pain, including intensity, frequency, constancy, predominance, predictability, duration, speed of onset and relationship to bowel movements. We evaluated the impact of each dimension on illness severity using multivariable regression techniques.
Results: Among the pain dimensions, intensity, frequency, constancy and predictability were strongly and independently associated with illness severity; the other dimensions had weaker associations. The clinical definition of 'pain predominance', in which patients define pain as their most bothersome symptom, was insufficient to categorize patients by illness severity.
Conclusions: Irritable bowel disease pain is multifaceted; some pain dimensions drive illness more than others. IBS trials should measure various pain dimensions, including intensity, constancy, frequency and predictability; this may improve upon the customary use of measuring pain as a unidimensional symptom in IBS.
© 2010 Blackwell Publishing Ltd.
Figures
References
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130:1480–91. - PubMed
-
- Whitehead WE, Crowell MD, Bosmajian L, et al. Existence of irritable bowel syndrome supported by factor analysis of symptoms in two community samples. Gastroenterology. 1990;98:336–40. - PubMed
-
- Taub E, Cuevas JL, Cook EW, III, Crowell M, Whitehead WE. Irritable bowel syndrome defined by factor analysis. Gender and race comparisons. Dig Dis Sci. 1995;40:2647–55. - PubMed
-
- Spiegel BM, Gralnek IM, Bolus R, et al. Clinical determinants of health-related quality of life in patients with irritable bowel syndrome. Arch Intern Med. 2004;164:1773–80. - PubMed