

Atrial fibrosis helps select the appropriate patient and strategy in catheter ablation of atrial fibrillation: a DE-MRI guided approach
- PMID: 20807271
- PMCID: PMC3133570
- DOI: 10.1111/j.1540-8167.2010.01876.x
Atrial fibrosis helps select the appropriate patient and strategy in catheter ablation of atrial fibrillation: a DE-MRI guided approach
Abstract
MRI for AF Patient Selection and Ablation Approach.
Introduction: Left atrial (LA) fibrosis and ablation related scarring are major predictors of success in rhythm control of atrial fibrillation (AF). We used delayed enhancement MRI (DE-MRI) to stratify AF patients based on pre-ablation fibrosis and also to evaluate ablation-induced scarring in order to identify predictors of a successful ablation.
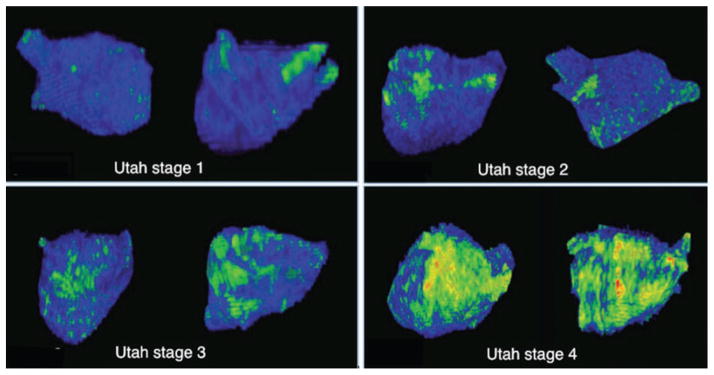
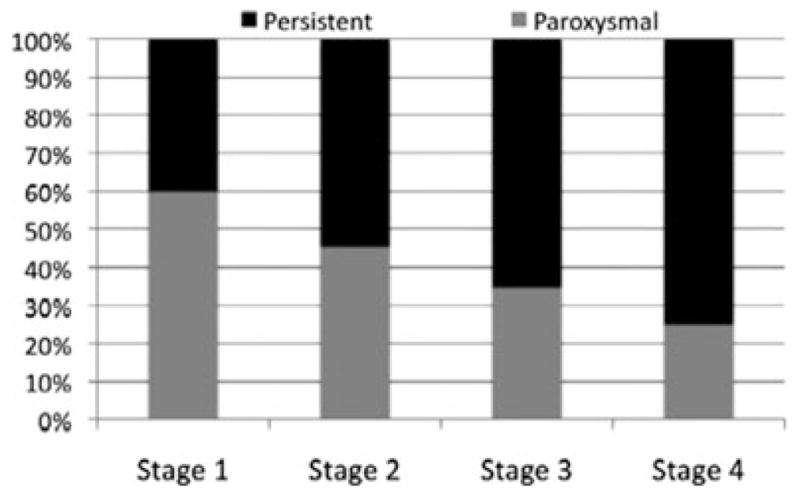
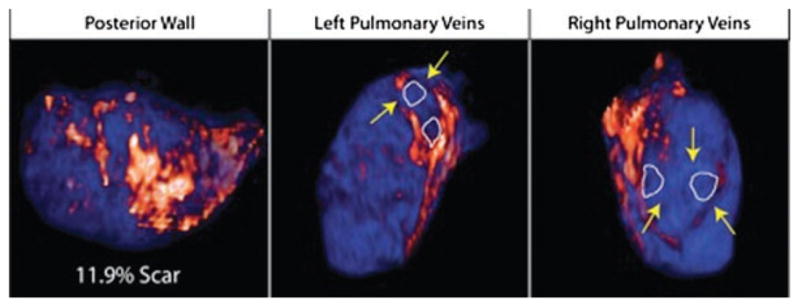
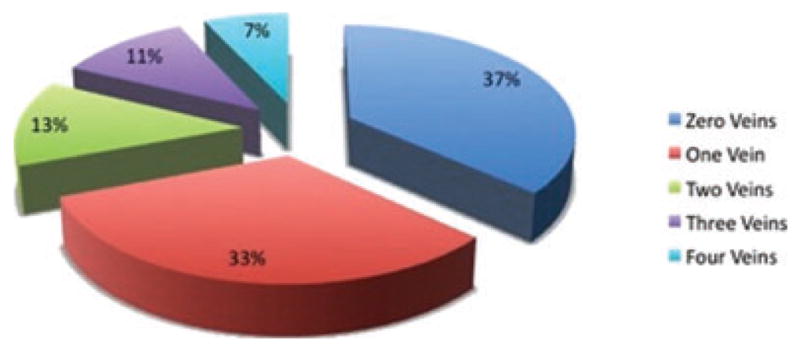
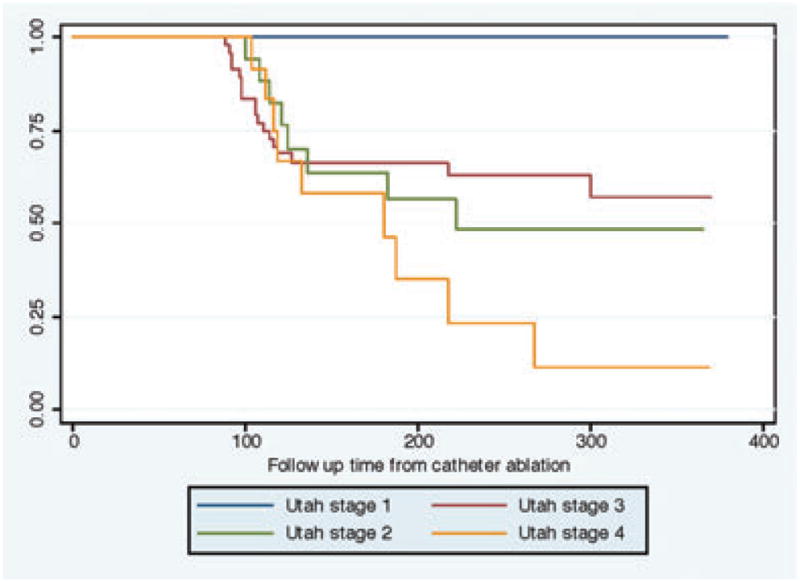
Methods and results: One hundred and forty-four patients were staged by percent of fibrosis quantified with DE-MRI, relative to the LA wall volume: minimal or Utah stage 1; <5%, mild or Utah stage 2; 5-20%, moderate or Utah stage 3; 20-35%, and extensive or Utah stage 4; >35%. All patients underwent pulmonary vein (PV) isolation and posterior wall and septal debulking. Overall, LA scarring was quantified and PV antra were evaluated for circumferential scarring 3 months post ablation. LA scarring post ablation was comparable across the 4 stages. Most patients had either no (36.8%) or 1 PV (32.6%) antrum circumferentially scarred. Forty-two patients (29%) had recurrent AF over 283 ± 167 days. No recurrences were noted in Utah stage 1. Recurrence was 28% in Utah stage 2, 35% in Utah stage 3, and 56% in Utah stage 4. Recurrence was predicted by circumferential PV scarring in Utah stage 2 and by overall LA wall scarring in Utah stage 3. No recurrence predictors were identified in Utah stage 4.
Conclusions: Circumferential PV antral scarring predicts ablation success in mild LA fibrosis, while posterior wall and septal scarring is needed for moderate fibrosis. This may help select the proper candidate and strategy in catheter ablation of AF.
© 2010 Wiley Periodicals, Inc.
Figures
Comment in
-
The role of MRI-detected left atrial delayed enhancement in selecting the right patient and choosing the optimal strategy for catheter ablation of atrial fibrillation.J Cardiovasc Electrophysiol. 2011 Jan;22(1):23-4. doi: 10.1111/j.1540-8167.2010.01904.x. Epub 2010 Sep 14. J Cardiovasc Electrophysiol. 2011. PMID: 20840463 No abstract available.
-
Prevention through intervention: catheter ablation to reduce the rate of progression of paroxysmal to persistent atrial fibrillation.J Cardiovasc Electrophysiol. 2012 Jan;23(1):15-7. doi: 10.1111/j.1540-8167.2011.02157.x. Epub 2011 Sep 2. J Cardiovasc Electrophysiol. 2012. PMID: 21895832 No abstract available.
References
-
- Fuster VRL, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC, Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Halperin JL, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Tamargo JL, Zamorano JL. American College of Cardiology; American Heart Association Task Force; European Society of Cardiology Committee for Practice Guidelines; European Heart Rhythm Association; Heart Rhythm Society: ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): Developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2007;114:e257–354. - PubMed
-
- Go ASHE, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk Factors in Atrial Fribrillation (ATRIA) Study. JAMA. 2001;285:2370–2375. - PubMed
-
- Ausma J, Wijffels M, Thone F, Wouters L, Allessie M, Borgers M. Structural changes of atrial myocardium due to sustained atrial fibrillation in the goat. Circulation. 1997;96:3157–3163. - PubMed
-
- Bosch RF, Zeng X, Grammer JB, Popovic K, Mewis C, Kühlkamp V. Ionic mechanisms of electrical remodeling in human atrial fibrillation. Cardiovascular Research. 1999;44:121–131. - PubMed
-
- Allessie MAJ, Schotten U. Electrical, contractile and structural remodeling during atrial fibrillation. Cardiovascular Research. 2002;54:230–236. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
