

Validity and test-retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients
- PMID: 20807405
- PMCID: PMC2942800
- DOI: 10.1186/1471-2474-11-194
Validity and test-retest reliability of manual goniometers for measuring passive hip range of motion in femoroacetabular impingement patients
Abstract
Background: The aims of this study were to evaluate the construct validity (known group), concurrent validity (criterion based) and test-retest (intra-rater) reliability of manual goniometers to measure passive hip range of motion (ROM) in femoroacetabular impingement patients and healthy controls.
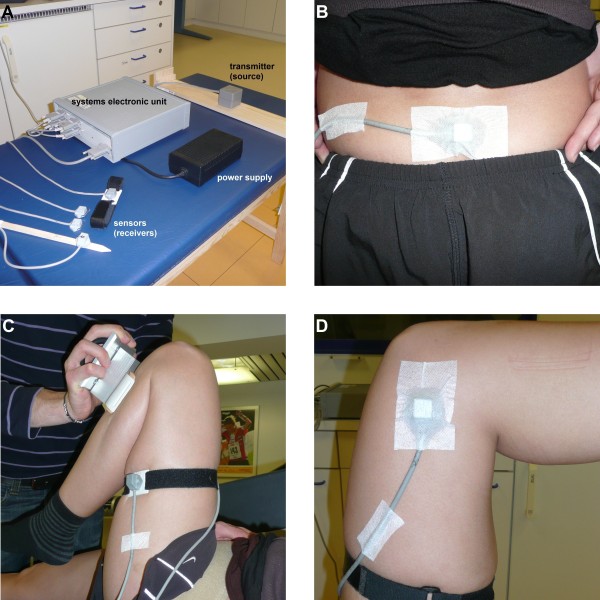
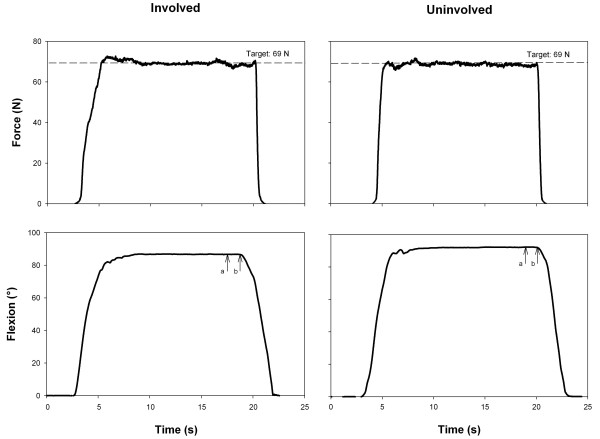
Methods: Passive hip flexion, abduction, adduction, internal and external rotation ROMs were simultaneously measured with a conventional goniometer and an electromagnetic tracking system (ETS) on two different testing sessions. A total of 15 patients and 15 sex- and age-matched healthy controls participated in the study.
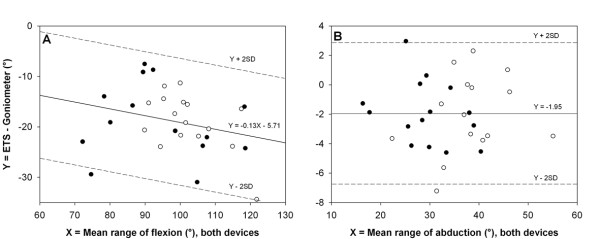
Results: The goniometer provided greater hip ROM values compared to the ETS (range 2.0-18.9 degrees; P < 0.001); good concurrent validity was only achieved for hip abduction and internal rotation, with intraclass correlation coefficients (ICC) of 0.94 and 0.88, respectively. Both devices detected lower hip abduction ROM in patients compared to controls (P < 0.01). Test-retest reliability was good with ICCs higher 0.90, except for hip adduction (0.82-0.84). Reliability estimates did not differ between the goniometer and the ETS.
Conclusions: The present study suggests that goniometer-based assessments considerably overestimate hip joint ROM by measuring intersegmental angles (e.g., thigh flexion on trunk for hip flexion) rather than true hip ROM. It is likely that uncontrolled pelvic rotation and tilt due to difficulties in placing the goniometer properly and in performing the anatomically correct ROM contribute to the overrating of the arc of these motions. Nevertheless, conventional manual goniometers can be used with confidence for longitudinal assessments in the clinic.
Figures

Similar articles
-
Combining results from hip impingement and range of motion tests can increase diagnostic accuracy in patients with FAI syndrome.Knee Surg Sports Traumatol Arthrosc. 2020 Oct;28(10):3382-3392. doi: 10.1007/s00167-020-06005-5. Epub 2020 Apr 25. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 32335699 Free PMC article.
-
Intratester and intertester reliability and criterion validity of the parallelogram and universal goniometers for active knee flexion in healthy subjects.Physiother Res Int. 1997;2(3):150-66. doi: 10.1002/pri.97. Physiother Res Int. 1997. PMID: 9421820 Review.
-
Is the Kinect system suitable for evaluation of the hip joint range of motion and as a screening tool for femoroacetabular impingement (FAI)?Technol Health Care. 2015;23(1):75-81. doi: 10.3233/THC-140870. Technol Health Care. 2015. PMID: 25391527 Clinical Trial.
-
Hip muscle weakness and reduced joint range of motion in patients with femoroacetabular impingement syndrome: a case-control study.Braz J Phys Ther. 2020 Jan-Feb;24(1):39-45. doi: 10.1016/j.bjpt.2018.11.010. Epub 2018 Nov 20. Braz J Phys Ther. 2020. PMID: 30509854 Free PMC article.
-
Does femoroacetabular impingement syndrome affect range of motion? A systematic review with meta-analysis.Br Med Bull. 2023 Apr 5;145(1):45-59. doi: 10.1093/bmb/ldac027. Br Med Bull. 2023. PMID: 36368014
Cited by
-
Shear elastic modulus is a reproducible index reflecting the passive mechanical properties of medial gastrocnemius muscle belly.Acta Radiol Open. 2016 Apr 28;5(4):2058460115604009. doi: 10.1177/2058460115604009. eCollection 2016 Apr. Acta Radiol Open. 2016. PMID: 27170845 Free PMC article.
-
An Anterior Cruciate Ligament (ACL) Injury Risk Screening and Reduction Program for High School Female Athletes: A Pilot Study.Int J Sports Phys Ther. 2022 Dec 1;17(7):1318-1329. doi: 10.26603/001c.40370. eCollection 2022. Int J Sports Phys Ther. 2022. PMID: 36518824 Free PMC article.
-
Asymptomatic Participants With a Femoroacetabular Deformity Demonstrate Stronger Hip Extensors and Greater Pelvis Mobility During the Deep Squat Task.Orthop J Sports Med. 2018 Jul 17;6(7):2325967118782484. doi: 10.1177/2325967118782484. eCollection 2018 Jul. Orthop J Sports Med. 2018. PMID: 30038915 Free PMC article.
-
Hip Range of Motion Is Increased After Hip Arthroscopy for Femoroacetabular Impingement: A Systematic Review.Arthrosc Sports Med Rehabil. 2022 Jan 22;4(2):e797-e822. doi: 10.1016/j.asmr.2021.12.001. eCollection 2022 Apr. Arthrosc Sports Med Rehabil. 2022. PMID: 35494261 Free PMC article. Review.
-
Combining results from hip impingement and range of motion tests can increase diagnostic accuracy in patients with FAI syndrome.Knee Surg Sports Traumatol Arthrosc. 2020 Oct;28(10):3382-3392. doi: 10.1007/s00167-020-06005-5. Epub 2020 Apr 25. Knee Surg Sports Traumatol Arthrosc. 2020. PMID: 32335699 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
