Antibodies in transplantation
- PMID: 20807473
- PMCID: PMC3056494
Antibodies in transplantation
Abstract
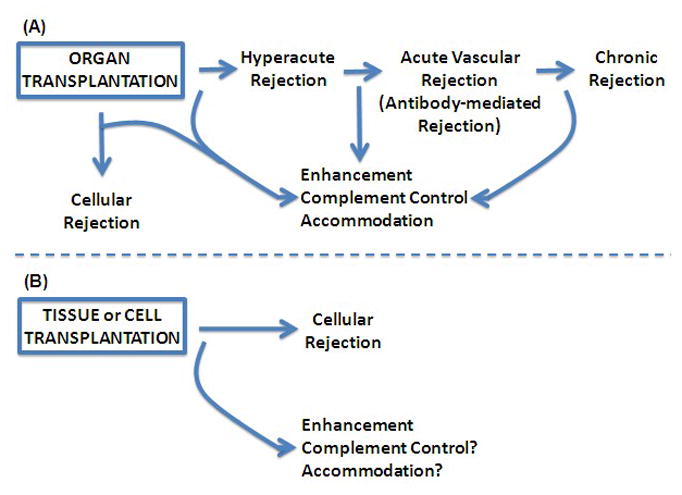
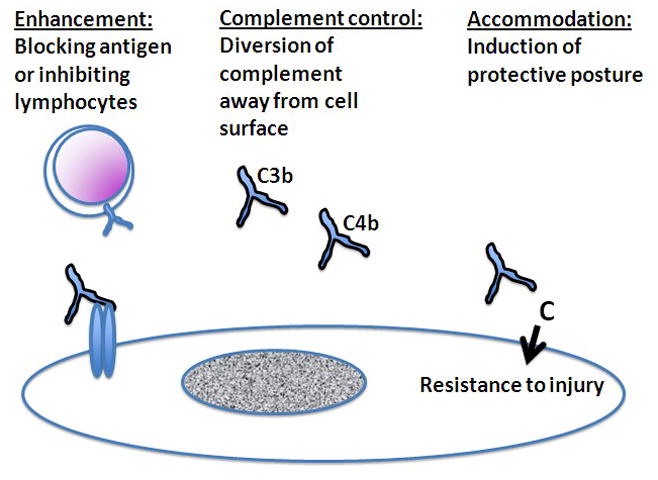
Transplantation of cells, tissues, and organs from one individual to another can incite the production of antibodies specific for foreign antigens, especially major histocompatibility antigens, in the graft. Antibodies specific for a graft provide an index of immunity and a potential trigger for injury and rejection. However, the index of immunity can sometimes miss antibody-mediated rejection and besides causing injury the antibodies against a graft can also protect a graft from injury by blocking immune recognition, called enhancement, regulating activation of complement, and inducing changes in the graft that resist damage. Reviewed here are potential limitations in the use of antibodies as an index of immunity and the ways antibodies cause and/or prevent injury.
Figures
Similar articles
-
Complement-activating donor-specific anti-HLA antibodies and solid organ transplant survival: A systematic review and meta-analysis.PLoS Med. 2018 May 25;15(5):e1002572. doi: 10.1371/journal.pmed.1002572. eCollection 2018 May. PLoS Med. 2018. PMID: 29799874 Free PMC article.
-
Transplantation immunology.Pediatr Clin North Am. 1994 Aug;41(4):819-39. doi: 10.1016/s0031-3955(16)38809-5. Pediatr Clin North Am. 1994. PMID: 8047371 Review.
-
[Lymphocytes in transplantation immunity--in the relation to HLA antigens].Hum Cell. 1988 Sep;1(3):275-81. Hum Cell. 1988. PMID: 2979204 Japanese.
-
The effect of MICA antigens on kidney transplantation outcomes.Immunol Lett. 2013 Nov-Dec;156(1-2):54-8. doi: 10.1016/j.imlet.2013.08.009. Epub 2013 Sep 1. Immunol Lett. 2013. PMID: 24004718 Review.
-
Utility of HLA Antibody Testing in Kidney Transplantation.J Am Soc Nephrol. 2015 Jul;26(7):1489-502. doi: 10.1681/ASN.2014080837. Epub 2015 Mar 24. J Am Soc Nephrol. 2015. PMID: 25804279 Free PMC article. Review.
Cited by
-
A common gene signature in tolerance to renal allograft.Kidney Int. 2015 Dec;88(6):1447-1448. doi: 10.1038/ki.2015.309. Kidney Int. 2015. PMID: 26649666 No abstract available.
-
ABO-compatible liver allograft antibody-mediated rejection: an update.Curr Opin Organ Transplant. 2015 Jun;20(3):314-24. doi: 10.1097/MOT.0000000000000194. Curr Opin Organ Transplant. 2015. PMID: 25944231 Free PMC article. Review.
-
IRF4 ablation in B cells abrogates allogeneic B cell responses and prevents chronic transplant rejection.J Heart Lung Transplant. 2021 Oct;40(10):1122-1132. doi: 10.1016/j.healun.2021.06.008. Epub 2021 Jun 23. J Heart Lung Transplant. 2021. PMID: 34253454 Free PMC article.
-
The impact of donor-specific anti-HLA antibodies on late kidney allograft failure.Nat Rev Nephrol. 2012 Apr 17;8(6):348-57. doi: 10.1038/nrneph.2012.81. Nat Rev Nephrol. 2012. PMID: 22508180 Review.
-
Donor specific antibodies after transplantation.Pediatr Transplant. 2011 Nov;15(7):686-90. doi: 10.1111/j.1399-3046.2010.01436.x. Epub 2011 Mar 29. Pediatr Transplant. 2011. PMID: 22004543 Free PMC article. Review.
References
-
- Alexandre GPJ, Squifflet JP, De Bruyere M, Latinne D, Moriau M, Ikabu N, Carlier M, Pirson Y. Splenectomy as a prerequisite for successful human ABO-incompatible renal transplantation. Transplant Proc. 1985;17:138–43.
-
- Andrejevic S, Bonaci-Nikolic B, Sefik-Bukilica M, Petrovic R. Clinical and serological follow-up of 71 patients with anti-mitochondrial type 5 antibodies. Lupus. 2007;16(10):788–93. - PubMed
-
- Bannett AD, Mcalack RF, Morris M, Chopek M, Platt JL. ABO incompatible renal transplantation: A qualitative analysis of native endothelial tissue ABO antigens after transplant. Transplant Proc. 1989;21:783–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources