

Vagoglossopharyngeal-associated syncope due to a retained bullet in the jugular foramen
- PMID: 20808535
- PMCID: PMC2853077
- DOI: 10.1055/s-0029-1225532
Vagoglossopharyngeal-associated syncope due to a retained bullet in the jugular foramen
Abstract
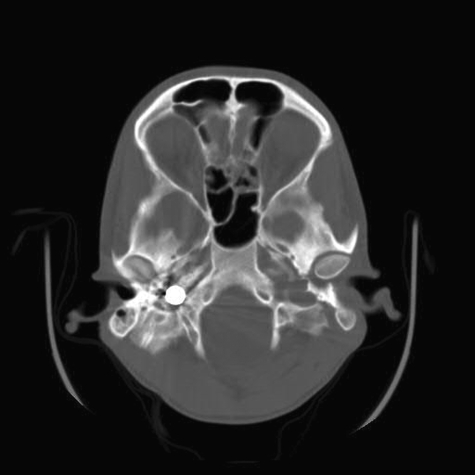
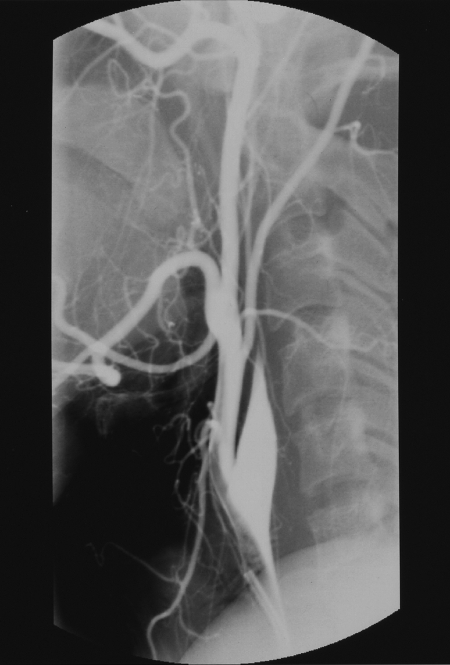
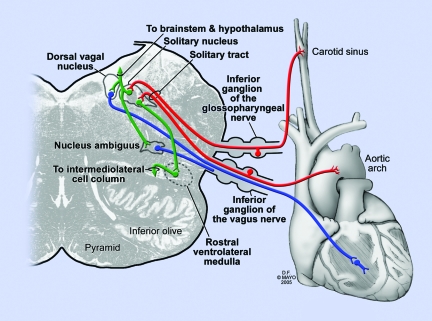
Gunshot wounds (GSWs) to the head are frequently fatal. Rarely, the bullet may lodge in the skull base and not cause significant brain injury. Typically, the bullet fragments are felt to be inert and do not require operative extirpation if they are within the bony confines of the skull base. We report the case of a bullet in the jugular foramen causing recurrent syncope that resolved after surgical removal of the bullet. The medical records from a patient who suffered a GSW to the head were retrospectively reviewed and the treatment and outcome documented. In 2000, a 20-year-old man suffered a GSW to the head. Immediate evaluation revealed the bullet in the right skull base at the jugular foramen, but no parenchymal brain injury. One year after the GSW, he began to experience stereotypical spells resulting in loss of consciousness. Extensive cardiovascular workup was normal. In 2002, the patient underwent removal of the bullet. He has been syncope-free since the operation and returned to his career in the military. We believe the retained bullet in this patient was irritating the IX-X cranial nerves, resulting in syncope, similar to the mechanism in vagoglossopharyngeal neuralgia. Removing the bullet relieved the irritation and stopped the syncopal spells.
Keywords: Gunshot wounds; Syncope; jugular foramen; vagoglossopharyngeal neuralgia.
Figures


Similar articles
-
Civilian gunshot wounds to the head: a case report, clinical management, and literature review.Chin Neurosurg J. 2021 Feb 3;7(1):12. doi: 10.1186/s41016-020-00227-9. Chin Neurosurg J. 2021. PMID: 33531086 Free PMC article.
-
Gunshot Wound to the Posterior Fossa With a Transcerebellar Retromesencepahlic Bullet Path, Transient Mutism, and Unexpected Functional Recovery: The Pivotal, Energy-Absorbing Function of the Petrous Bone and Tentorial Leaflet.Cureus. 2023 Apr 11;15(4):e37420. doi: 10.7759/cureus.37420. eCollection 2023 Apr. Cureus. 2023. PMID: 37182019 Free PMC article.
-
Sinking bullet syndrome: A unique case of transhemispheric migration.Clin Neurol Neurosurg. 2021 May;204:106607. doi: 10.1016/j.clineuro.2021.106607. Epub 2021 Mar 20. Clin Neurol Neurosurg. 2021. PMID: 33774506
-
Pediatric Gunshot Wound to Visual Cortex with Retained Bullet: Case Report and Review of the Literature.Pediatr Neurosurg. 2021;56(1):94-98. doi: 10.1159/000513100. Epub 2021 Jan 29. Pediatr Neurosurg. 2021. PMID: 33517340 Review.
-
Removal of Migrating Lumbar Spine Bullet: Case Report and Surgical Video.World Neurosurg. 2019 Nov;131:62-64. doi: 10.1016/j.wneu.2019.07.151. Epub 2019 Jul 26. World Neurosurg. 2019. PMID: 31356981 Review.
Cited by
-
Examination of metal mobilization from a gunshot by scanning acoustic microscopy, scanning electron microscopy, energy-dispersive X-ray spectroscopy, and inductively coupled plasma optical emission spectroscopy: a case report.J Med Case Rep. 2018 Dec 28;12(1):391. doi: 10.1186/s13256-018-1905-7. J Med Case Rep. 2018. PMID: 30593288 Free PMC article.
-
A Potentially Dangerous Industrial Projectile Lodged in the Leg of a Steel Factory Worker.Cureus. 2021 Sep 10;13(9):e17870. doi: 10.7759/cureus.17870. eCollection 2021 Sep. Cureus. 2021. PMID: 34660071 Free PMC article.
-
Skeletal sarcoma on the site of retained war bullet fragments and a literature review on long-term complications of retained war shells.Arch Bone Jt Surg. 2013 Dec;1(2):107-11. Epub 2013 Dec 15. Arch Bone Jt Surg. 2013. PMID: 25207300 Free PMC article.
References
-
- Koop C E, Lundberg G B. Violence in America: a public health emergency. Time to bite the bullet back. JAMA. 1992;267:3075–3076. - PubMed
-
- Richmond T S, Lemaire J. Years of life lost because of gunshot injury to the brain and spinal cord. Am J Phys Med Rehabil. 2008;87:609–615. quiz 615–618. - PubMed
-
- Kennedy F, Gonzalez P, Dang C, Fleming A, Sterling-Scott R. The Glasgow Coma Scale and prognosis in gunshot wounds to the brain. J Trauma. 1993;35:75–77. - PubMed
-
- Kaufman H H, Makela M E, Lee K F, Haid R W, Jr, Gildenberg P L. Gunshot wounds to the head: a perspective. Neurosurgery. 1986;18:689–695. - PubMed
-
- Part 2: Prognosis in penetrating brain injury. J Trauma. 2001;51(2 suppl):S44–S86. - PubMed
