

Complications from injectable materials used for breast augmentation
- PMID: 20808751
- PMCID: PMC2740603
- DOI: 10.1177/229255030901700305
Complications from injectable materials used for breast augmentation
Abstract
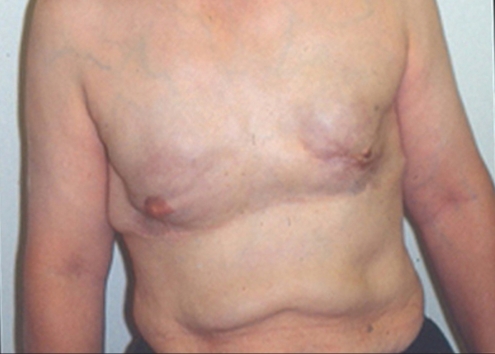
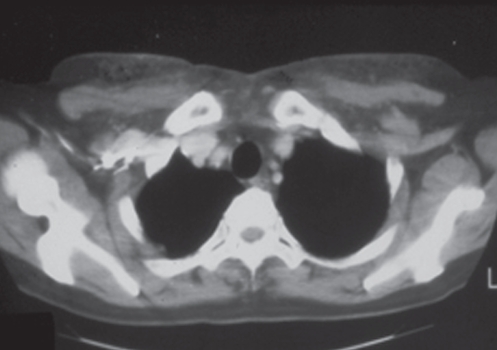
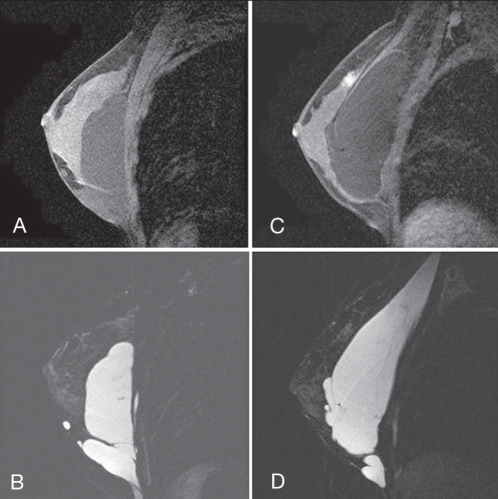
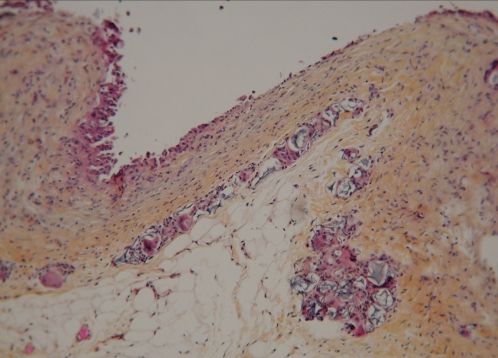
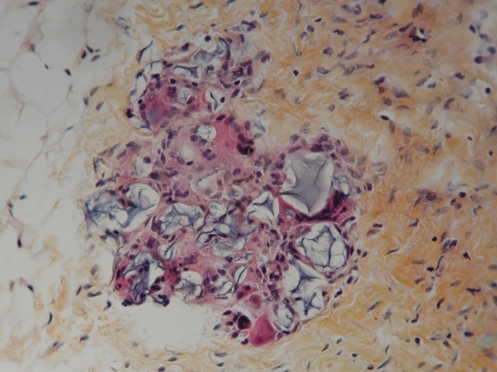
Fewer surgical procedures have a history as fascinating and as terrifying as breast augmentation. Initial efforts at augmentation involved injection of substances such as paraffin or oil into the breast tissue, or the implantation of substances including ivory or glass balls, or rubber. More recent efforts have included the injection of liquid silicone or polyacrylamide hydrogel. The current paper reviews four distinct eras of breast augmentation, and provides the current status of these injection materials. A case report is presented on a woman whose breasts were injected with polyacrylamide hydrogel in Iran. The current status of this group of materials is also presented. During the past 110 years, history has repeated itself during each of the four eras of injection.
Peu de techniques chirurgicales ont une histoire à la fois aussi fascinante et terrifiante que l’augmentation mammaire. Les premières tentatives ont porté sur l’injection de substances (paraffine, huile) ou sur l’implantation de matériaux (boules d’ivoire ou de verre, caoutchouc) dans les tissus mammaires. Plus récemment, on a procédé à des injections de silicone liquide ou d’hydrogel de polyacrylamide. Le présent article passe en revue les quatre époques de l’histoire de l’augmentation mammaire et nous dit où en est actuellement l’utilisation de ces injections. Il fait état d’un rapport de cas d’augmentation mammaire par injection d’hydrogel de polyacrylamide en Iran et fait également le point sur cette catégorie de substance. Au cours des 110 dernières années, l’histoire des injections s’est répétée, à chacune des quatre étapes.
Keywords: Breast; Injectable; Liquid silicone; Paraffin; Polyacrylamide hydrogel.
Figures






References
-
- Gersuny R. Ueber eine subcutyane Prothese. Z Heilk. 1900;30:1–5.
-
- Gersuny R. Harte and weiche Paraffinprothesen. Zentralbl Chir. 1903;30:1–3.
-
- Hollander E. Abstract from Berliner Gesellschaft fur Chirurgie. Munch Med Wochenschr. 1912;59:2842.
-
- Kolle FS. Plastic and Cosmetic Surgery. New York: D Appleton and Co; 1911.
-
- Schmorl Paraffingranulome, Munch Med Wochenscr. 1922;69:215–20.
LinkOut - more resources
Full Text Sources
Miscellaneous