

Airway remodelling in asthma: from benchside to clinical practice
- PMID: 20808979
- PMCID: PMC2933777
- DOI: 10.1155/2010/318029
Airway remodelling in asthma: from benchside to clinical practice
Abstract
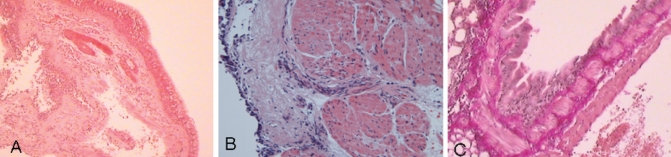
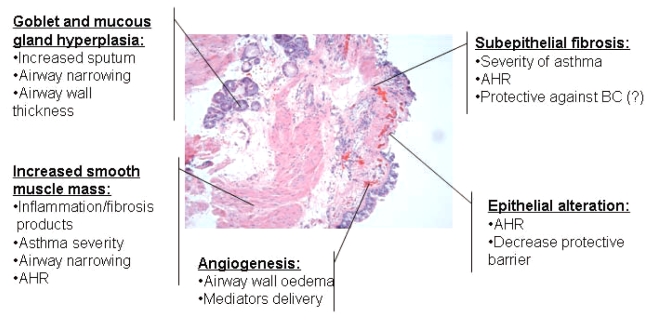
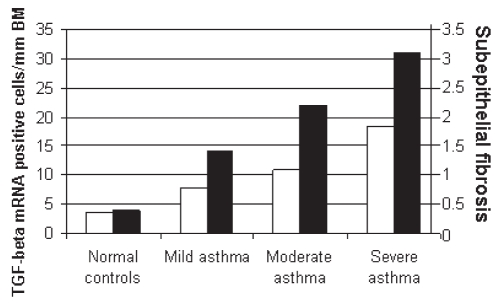
Airway remodelling refers to the structural changes that occur in both large and small airways relevant to miscellaneous diseases including asthma. In asthma, airway structural changes include subepithelial fibrosis, increased smooth muscle mass, gland enlargement, neovascularization and epithelial alterations. Although controversial, airway remodelling is commonly attributed to an underlying chronic inflammatory process. These remodelling changes contribute to thickening of airway walls and, consequently, lead to airway narrowing, bronchial hyper-responsiveness, airway edema and mucous hypersecretion. Airway remodelling is associated with poor clinical outcomes among asthmatic patients. Early diagnosis and prevention of airway remodelling has the potential to decrease disease severity, improve control and prevent disease expression. The relationship between structural changes and clinical and functional abnormalities clearly deserves further investigation. The present review briefly describes the characteristic features of airway remodelling observed in asthma, its clinical consequences and relevance for physicians, and its modulation by therapeutic approaches used in the treatment of asthmatic patients.
Le remodelage des voies respiratoires fait référence aux changements structuraux qui affectent les voies respiratoires, de gros et de petit volume, en lien avec diverses maladies, dont l’asthme. Dans l’asthme, les changements structuraux des voies respiratoires incluent la fibrose sous-épithéliale, l’augmentation de la masse musculaire lisse, l’hypertrophie glandulaire, la néovascularisation et des altérations épithéliales. Bien qu’il ne fasse pas l’unanimité, le remodelage des voies respiratoires est souvent attribué à un processus inflammatoire chronique sous-jacent. Ces anomalies contribuent à l’épaississement de la paroi des voies respiratoires et par conséquent, à un rétrécissement de leur calibre, à une hyperréactivité bronchique, à l’œdème et à l’hypersécrétion. Le remodelage des voies respiratoires est associé à de piètres paramètres cliniques chez les patients asthmatiques. Le dépistage précoce et la prévention du remodelage des voies respiratoires peuvent atténuer la gravité de la maladie, en améliorer la maîtrise et en prévenir l’expression. Le lien entre les changements structuraux et les anomalies cliniques et fonctionnelles mérite clairement qu’on s’y attarde davantage. La présente synthèse décrit brièvement les caractéristiques clés du remodelage des voies respiratoires observées dans l’asthme, leurs conséquences cliniques, leur portée sur la pratique médicale et leur modulation au moyen des approches thérapeutiques antiasthmatiques.
Figures
References
-
- James AL, Maxwell PS, Pearce-Pinto G, Elliot JG, Carroll NG. The relationship of reticular basement membrane thickness to airway wall remodeling in asthma. Am J Respir Crit Care Med. 2002;166:1590–5. - PubMed
-
- Roche WR, Beasley R, Williams JH, Holgate ST. Subepithelial fibrosis in the bronchi of asthmatics. Lancet. 1989;1:520–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
