

Incidence of rearrest after return of spontaneous circulation in out-of-hospital cardiac arrest
- PMID: 20809686
- PMCID: PMC3226713
- DOI: 10.3109/10903127.2010.497902
Incidence of rearrest after return of spontaneous circulation in out-of-hospital cardiac arrest
Abstract
Background: Return of spontaneous circulation (ROSC) occurs in 35.0 to 61.0% of emergency medical services (EMS)-treated out-of-hospital cardiac arrests (OHCAs); however, not all patients achieving ROSC survive to hospital arrival or discharge. Previous studies have estimated the incidence of some types of rearrest(RA) at 61.0 to 79.0%, and the electrocardiogram (ECG) waveform characteristics of prehospital RA rhythms have not been previously described.
Objectives: We sought to determine the incidence of RA in OHCA, to classify RA events by type, and to measure the time from ROSC to RA. We also conducted a preliminary analysis of the relationship between first EMS-detected rhythms and RA, as well as the effect of RA on survival.
Methods: The Pittsburgh Regional Clinical Center of the National Heart, Lung, and Blood Institute (NHLBI) -sponsored Resuscitation Outcomes Consortium (ROC) provided cases from a population-based cardiac arrest surveillance program, ROC Epistry. Only OHCA cases of nontraumatic etiology with available and adequate ECG files were included. We analyzed defibrillator-monitor ECG tracings (Philips MRX), patient care reports (PCRs), and defibrillator audio recordings from EMS-treated cases of OHCA spanning the period from October 2006 to December 2008. We identified ROSC and RA through interpretation of ECG tracings and audio recordings. Rearrest events were categorized as ventricular fibrillation (VF), pulseless ventricular tachycardia (VT), asystole, and pulseless electrical activity (PEA) based on ECG waveform characteristics. Proportions of RA rhythms were stratified by first EMS rhythm and compared using Pearson's chi-square test. Logistic regression was used to test the predictive relationship between RA and survival to hospital discharge.
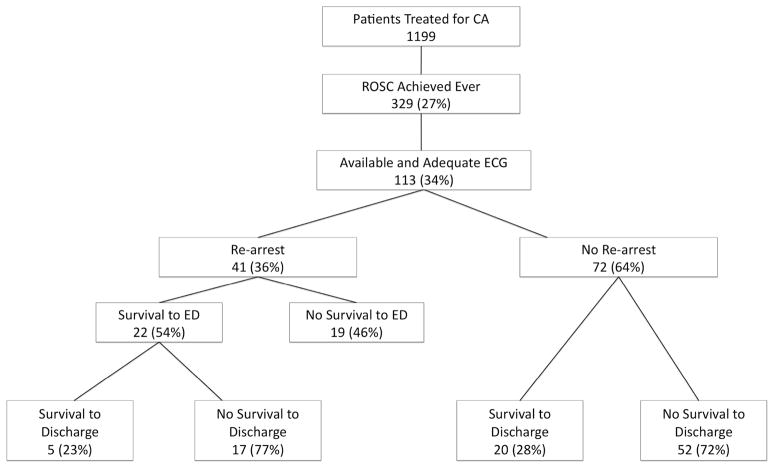
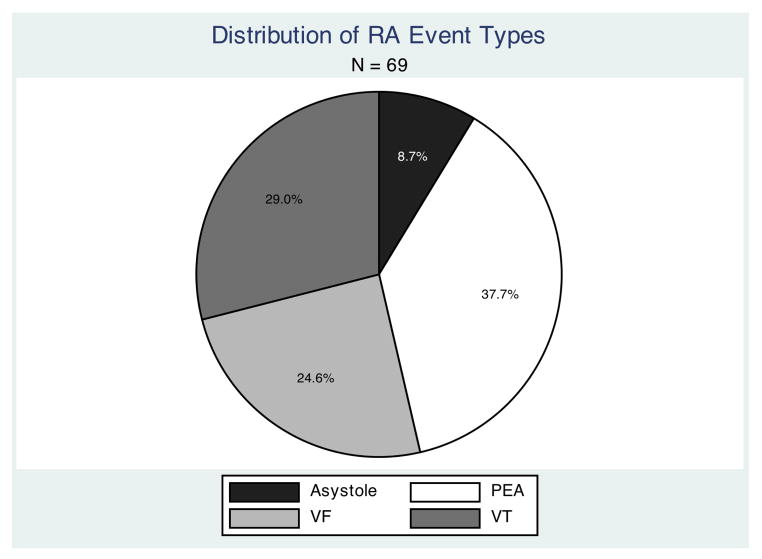
Results: Return of spontaneous circulation occurred in 329 of 1,199 patients (27.4% [95.0% confidence interval (CI): 25.0-30.0%]) treated for cardiac arrest. Of these, 113 had ECG tracings that were available and adequate for analysis. Rearrest occurred in 41 patients (36.0% [95.0% CI: 26.0-46.0%]), with a total of 69 RA events. Survival to hospital discharge in RA cases was 23.1% (95.0% CI: 11.1-39.3%), compared with 27.8% (95.0% CI: 17.9-39.6%) in cases without RA. Counts of RA events by type were as follows: 17 VF (24.6% [95% CI: 15.2-36.5%]), 20 pulseless VT (29.0% [95.0% CI: 18.7-41.2%]), 26 PEA (37.0% [95.0% CI: 26.3-50.2%]), and six asystole (8.8% [95.0% CI: 3.3-18.0%]). Rearrest was not predictive of survival to hospital discharge; however, initial EMS rhythm was predictive of RA shockability. The overall median (interquartile range) time from ROSC to RA among all events was 3.1 (1.6-6.3) minutes.
Conclusion: In this sample, the incidence of RA was 38.0%. The most common type of RA was PEA. Shockability of first EMS rhythm was found to predict subsequent RA rhythm shockability.
Figures
References
-
- Nichol G, Stiell IG, Laupacis A, Ba’Pham De Maio V, Wells G. A cumulative meta-analysis of the effectiveness of defibrillator-capable emergency medical services for victims of out-of-hospital cardiac arrest. Ann Emerg Med. 1999;34(4.1):517–525. - PubMed
-
- Gräsner JT, Meybohm P, Fischer M, Bein B, Wnent J, Franz R, Zander J, Lemke H, Bahr J, Jantzen T, Messelken M, Dörges V, Böttiger BW, Scholz J. A national resuscitation registry of out-of-hospital cardiac arrest in Germany-a pilot study. Resuscitation. 2009 Feb;80(2):199–203. - PubMed
-
- Grmec S, Krizmaric M, Mally S, Kozelj A, Spindler M, Lesnik B. Utstein style analysis of out-of-hospital cardiac arrest--bystander CPR and end expired carbon dioxide. Resuscitation. 2007 Mar;72(3):404–14. - PubMed
-
- White R, Russell J. Refibrillation, resuscitation and survival in out-of-hospital sudden cardiac arrest victims treated with biphasic automated external defibrillators. Resuscitation. 2002;55:17–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical