

Reinfection following initial cerebrospinal fluid shunt infection
- PMID: 20809713
- PMCID: PMC2953872
- DOI: 10.3171/2010.5.PEDS09457
Reinfection following initial cerebrospinal fluid shunt infection
Abstract
Object: Significant variation exists in the surgical and medical management of CSF shunt infection. The objectives of this study were to determine CSF shunt reinfection rates following initial CSF shunt infection in a large patient cohort and to determine management, patient, hospital, and surgeon factors associated with CSF shunt reinfection.
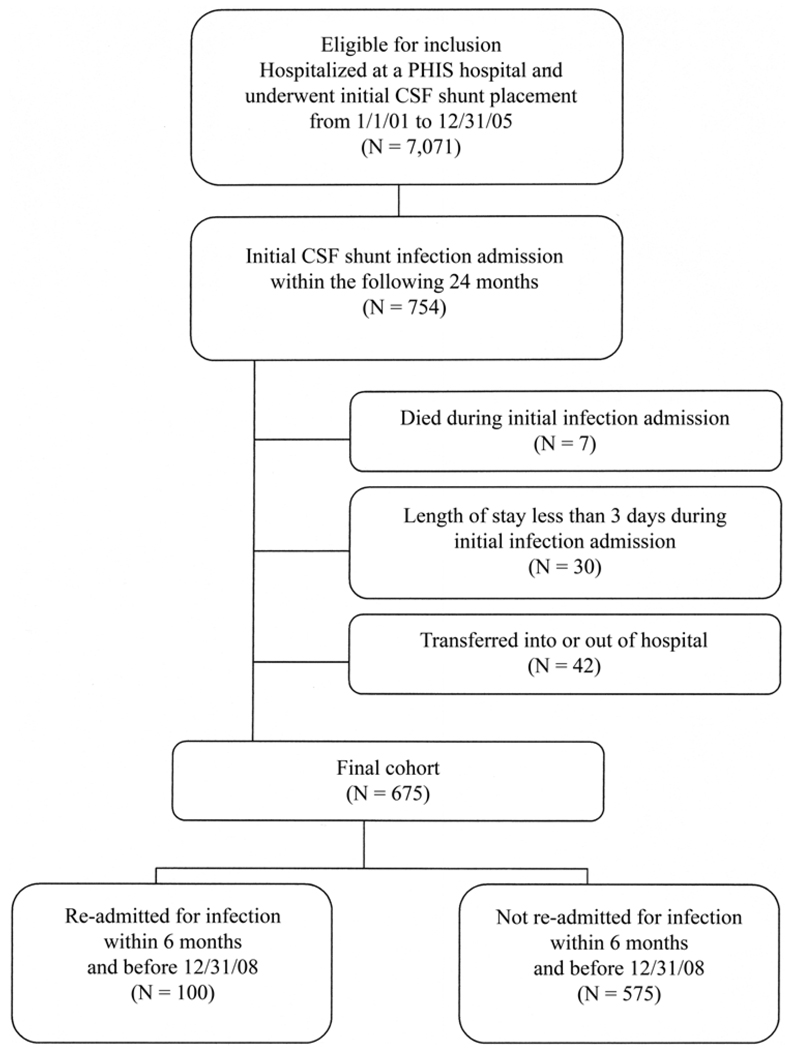
Methods: This retrospective cohort study included children who were in the Pediatric Health Information System (PHIS) database, who ranged in age from 0 to 18 years, and who underwent uncomplicated initial CSF shunt placement in addition to treatment for initial CSF shunt infection between January 1, 2001, and December 31, 2008. The outcome was CSF shunt reinfection within 6 months. The main predictor variable of interest was surgical approach to treatment of first infection, which was determined for 483 patients. Covariates included patient, hospital, surgeon, and other management factors.
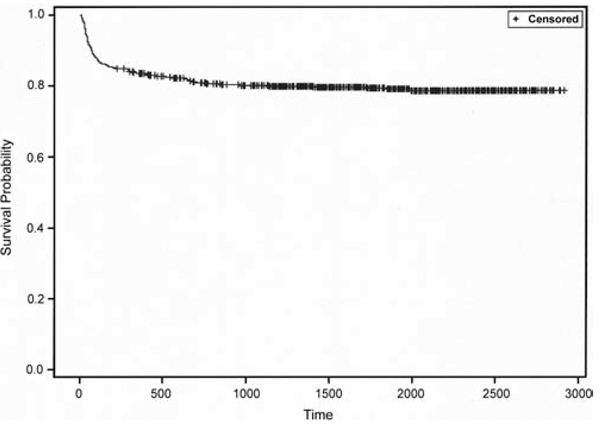
Results: The PHIS database includes 675 children with initial CSF shunt infection. Surgical approach to treatment of the initial CSF shunt infection was determined for 483 children (71.6%). The surgical approach was primarily shunt removal/new shunt placement (in 286 children [59.2%]), but a substantial number underwent externalization (59 children [12.2%]), of whom a subset went on to have the externalized shunt removed and a new shunt placed (17 children [3.5% overall]). Other approaches included nonsurgical management (64 children [13.3%]) and complete shunt removal without shunt replacement (74 children [15.3%]). The 6-month reinfection rate was 14.8% (100 of 675 patients). The median time from infection to reinfection was 21 days (interquartile range [IQR] 5-58 days). Children with reinfection had less time between shunt placement and initial infection (median 50 vs 79 days, p = 0.06). No differences between those with and without reinfection were seen in patient factors (patient age at either shunt placement or initial infection, sex, race/ethnicity, payer, indication for shunt, number of comorbidities, distal shunt location, and number of shunt revisions at first infection); hospital volume; surgeon volume; or other management factors (for example, duration of intravenous antibiotic use). Nonsurgical management was associated with reinfection, and complete shunt removal was negatively associated with reinfection. However, reinfection rates did not differ between the 2 most common surgical approaches: shunt removal/new shunt placement (44 [15.4%] of 286; 95% CI 11.4%-20.1%) and externalization (total 12 [20.3%] of 59; 95% CI 11.0%-32.8%). Externalization followed by shunt removal/new shunt placement (5 [29.4%] of 17; 95% CI 10.3%-56.0%) and nonsurgical management (15 [23.4%] of 64; 95% CI 13.8%-35.7%) had higher, but nonstatistically significant, reinfection rates. The length of stay was shorter for nonsurgical management.
Conclusions: Surgical approach to treatment of initial CSF shunt infection was not associated with reinfection in this large cohort of patients.
Figures
Similar articles
-
Reinfection after treatment of first cerebrospinal fluid shunt infection: a prospective observational cohort study.J Neurosurg Pediatr. 2018 Apr;21(4):346-358. doi: 10.3171/2017.9.PEDS17112. Epub 2018 Feb 2. J Neurosurg Pediatr. 2018. PMID: 29393813 Free PMC article.
-
Infection rates following initial cerebrospinal fluid shunt placement across pediatric hospitals in the United States. Clinical article.J Neurosurg Pediatr. 2009 Aug;4(2):156-65. doi: 10.3171/2009.3.PEDS08215. J Neurosurg Pediatr. 2009. PMID: 19645551 Free PMC article.
-
Management of shunt infections: a multicenter pilot study.J Neurosurg. 2006 Sep;105(3 Suppl):177-81. doi: 10.3171/ped.2006.105.3.177. J Neurosurg. 2006. PMID: 16970229
-
Association of intraventricular hemorrhage secondary to prematurity with cerebrospinal fluid shunt surgery in the first year following initial shunt placement.J Neurosurg Pediatr. 2012 Jan;9(1):54-63. doi: 10.3171/2011.10.PEDS11307. J Neurosurg Pediatr. 2012. PMID: 22208322 Free PMC article.
-
Progression of cerebrospinal fluid cell count and differential over a treatment course of shunt infection.J Neurosurg Pediatr. 2011 Dec;8(6):613-9. doi: 10.3171/2011.8.PEDS11236. J Neurosurg Pediatr. 2011. PMID: 22132920 Review.
Cited by
-
A search for bacteria identified from cerebrospinal fluid shunt infections in previous surgical events.PLoS One. 2024 Oct 10;19(10):e0311605. doi: 10.1371/journal.pone.0311605. eCollection 2024. PLoS One. 2024. PMID: 39388396 Free PMC article.
-
Action of linezolid or vancomycin on biofilms in ventriculoperitoneal shunts in vitro.Antimicrob Agents Chemother. 2012 Jun;56(6):2842-5. doi: 10.1128/AAC.06326-11. Epub 2012 Mar 19. Antimicrob Agents Chemother. 2012. PMID: 22430965 Free PMC article.
-
Molecular Characterization of Microbiota in Cerebrospinal Fluid From Patients With CSF Shunt Infections Using Whole Genome Amplification Followed by Shotgun Sequencing.Front Cell Infect Microbiol. 2021 Aug 20;11:699506. doi: 10.3389/fcimb.2021.699506. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 34490140 Free PMC article.
-
Management of Recurrent Ventriculoperitoneal Shunt Infections in Adult Patients.Antibiotics (Basel). 2025 Jan 13;14(1):77. doi: 10.3390/antibiotics14010077. Antibiotics (Basel). 2025. PMID: 39858363 Free PMC article.
-
Treatment and microbiology of repeated cerebrospinal fluid shunt infections in children.Pediatr Infect Dis J. 2011 Sep;30(9):731-5. doi: 10.1097/INF.0b013e318218ac0e. Pediatr Infect Dis J. 2011. PMID: 21852762 Free PMC article.
References
-
- Albert JE, Simon TD, Hall M, Kestle J, Jeffries HE. Pediatric Academic Societies Annual Meeting. Honolulu, Hawaii: 2008. May 2–6, Improved identification of pediatric neurosurgical procedure infections. (Abstract)
-
- Bayston R, Barnicoat M, Cudmore RE, Guiney EJ, Gurusinghe N, Norman PM. The use of intraventricular vancomycin in the treatment of CSF shunt-associated ventriculitis. Z Kinderchir. 1984;39 Suppl 2:111–113. - PubMed
-
- Brown EM, Edwards RJ, Pople IK. Conservative management of patients with cerebrospinal fluid shunt infections. Neurosurgery. 2006;58:657–665. - PubMed
-
- Cruciani M, Navarra A, Di Perri G, Andreoni M, Danzi MC, Concia E, et al. Evaluation of intraventricular teicoplanin for the treatment of neurosurgical shunt infections. Clin Infect Dis. 1992;15:285–289. - PubMed
-
- Fan-Havard P, Nahata MC. Treatment and prevention of infections of cerebrospinal fluid shunts. Clin Pharm. 1987;6:866–880. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
