

Uncemented custom femoral components in hip arthroplasty. A prospective clinical study of 191 hips followed for at least 7 years
- PMID: 20809741
- PMCID: PMC2917564
- DOI: 10.3109/17453674.2010.501748
Uncemented custom femoral components in hip arthroplasty. A prospective clinical study of 191 hips followed for at least 7 years
Abstract
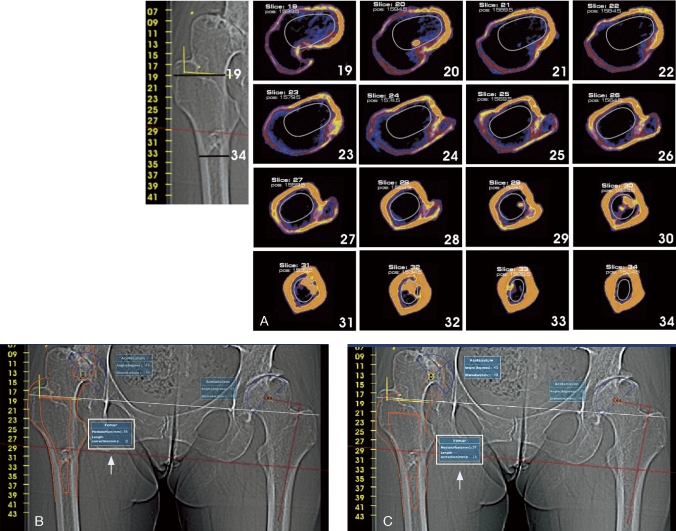
Background and purpose: We have developed an individually designed, uncemented femoral component for achievement of improved strain distribution and fixation to the bone, to make uncemented stems more applicable in femurs of abnormal size and shape, and to improve the joint mechanics. Here we describe the design of the implant and present the results of a prospective clinical study with at least 7 years of follow-up.
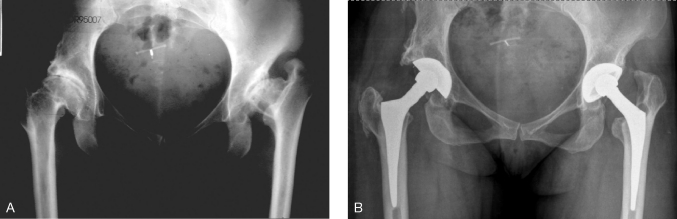
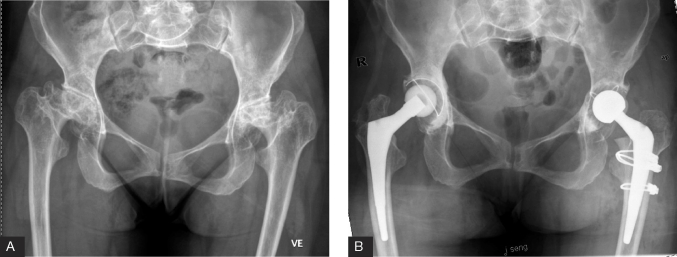
Patients and methods: The prostheses are produced by CAD-CAM technique. The design of the stem is based on CT information, and the neck design is based on the surgeon's planning of the center of rotation, femoral head offset, and leg length correction. The first-generation stem produced before 2001 had a proximal HA coating and a sand-blasted distal part that was down-scaled to avoid contact with compact bone. The second-generation stem had a porous coating beneath the HA layer and the distal part of the stem was polished. The implant was used in 762 hips (614 patients) from 1995 until 2009. 191 of these hips were followed for 7 years and 83 others were followed for 10 years, and these hips are included in the present study. Mean age at surgery was 48 (20-65) years. Congenital dysplasia of the hip was the reason for osteoarthritis in 46% and 57% of the hips in respective groups. Merle d'Aubigné score was recorded in 152 and 75 hips in the two groups. Prostheses followed for 10 years, and almost all in the 7-year group, were first-generation stems.
Results: The 7- and 10-year cumulative revision rates were 1.1% and 2.4%, respectively, with stem revision for any reason as endpoint. The clinical results were similar at 7 and 10 years, with Merle d'Aubigné scores of 17. Intraoperative trochanteric fissures occurred in 2 of the 191 operations (1.0%); both healed after wiring. In hips followed for 7 years, 2 periprosthetic fractures occurred; exchange of the stem was necessary in both. One additional fracture occurred between 7 and 10 years, and it was treated successfully with osteosynthesis. The rate of dislocation was 1.6% and 2.4%, respectively. There was no radiographic loosening at follow-up.
Interpretation: Use of a custom femoral stem gives a reliable fixation and promising medium-term clinical results in femurs of normal and abnormal shape and dimension. The individual design, which enables optimized joint mechanics, gives a low risk of mechanical complications.
Figures
Similar articles
-
One-third of Hips After Periacetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA.Clin Orthop Relat Res. 2017 Apr;475(4):1154-1168. doi: 10.1007/s11999-016-5169-5. Clin Orthop Relat Res. 2017. PMID: 27905061 Free PMC article.
-
High rate of fracture in the cementless modular Extrême™ (Mark I) femoral prosthesis in revision total hip arthroplasty: 33 cases at more than 5 years' follow-up.Orthop Traumatol Surg Res. 2013 Dec;99(8):915-21. doi: 10.1016/j.otsr.2013.08.007. Epub 2013 Nov 7. Orthop Traumatol Surg Res. 2013. PMID: 24211127
-
Effect of hydroxyapatite coating on the radio-clinical results of a grit-blasted titanium alloy femoral taper. A case-control study of 198 cementless primary total hip arthroplasty with the Alloclassic™ system.Orthop Traumatol Surg Res. 2014 Nov;100(7):739-44. doi: 10.1016/j.otsr.2014.07.010. Epub 2014 Sep 30. Orthop Traumatol Surg Res. 2014. PMID: 25261173
-
Long-term survivorship of the Corail™ standard stem.Orthop Traumatol Surg Res. 2017 Nov;103(7):987-992. doi: 10.1016/j.otsr.2017.06.010. Epub 2017 Aug 1. Orthop Traumatol Surg Res. 2017. PMID: 28778624
-
Total hip arthroplasty survival in femoral head avascular necrosis versus primary hip osteoarthritis: Case-control study with a mean 10-year follow-up after anatomical cementless metal-on-metal 28-mm replacement.Orthop Traumatol Surg Res. 2016 Dec;102(8):1029-1034. doi: 10.1016/j.otsr.2016.08.021. Epub 2016 Oct 27. Orthop Traumatol Surg Res. 2016. PMID: 28341264
Cited by
-
Bioelectronic multifunctional bone implants: recent trends.Bioelectron Med. 2022 Sep 21;8(1):15. doi: 10.1186/s42234-022-00097-9. Bioelectron Med. 2022. PMID: 36127721 Free PMC article. Review.
-
Outcomes of primary total hip arthroplasty using 3D image-based custom stems in unselected patients: a systematic review.EFORT Open Rev. 2021 Dec 10;6(12):1166-1180. doi: 10.1302/2058-5241.6.210053. EFORT Open Rev. 2021. PMID: 35767431 Free PMC article.
-
Periprosthetic bone loss after insertion of an uncemented, customized femoral stem and an uncemented anatomical stem. A randomized DXA study with 5-year follow-up.Acta Orthop. 2011 Aug;82(4):410-6. doi: 10.3109/17453674.2011.588860. Epub 2011 Jun 14. Acta Orthop. 2011. PMID: 21668387 Free PMC article. Clinical Trial.
-
Small and similar amounts of micromotion in an anatomical stem and a customized cementless femoral stem in regular-shaped femurs. A 5-year follow-up randomized RSA study.Acta Orthop. 2014 Apr;85(2):152-8. doi: 10.3109/17453674.2014.899846. Acta Orthop. 2014. PMID: 24650024 Free PMC article. Clinical Trial.
-
Bone Regeneration Based on Tissue Engineering Conceptions - A 21st Century Perspective.Bone Res. 2013 Sep 25;1(3):216-48. doi: 10.4248/BR201303002. eCollection 2013 Sep. Bone Res. 2013. PMID: 26273505 Free PMC article. Review.
References
-
- Aamodt A, Kvistad KA, Andersen E, Lund-Larsen J, Eine J, Benum P, Schnell Husby O. Determination of the Hounsfield value for CT-based design of custom femoral stems. J Bone Joint Surg (Br) 1999;81:143–7. - PubMed
-
- Aamodt A, Lund-Larsen J, Eine J, Andersen E, Benum P, Schnell Husby O. Changes in proximal femoral strains following insertion of uncemented standard and custom femoral stems. An experimental study in human femurs. J Bone Joint Surg (Br) 2001;83((6)):921–9. - PubMed
-
- Aamodt A, Lund-Larsen J, Eine J, Andersen E, Benum P, Schnell Husby O. Mechanical stability of custom and anatomical femoral stems. An experimental study in human femora. Hip International. 2002;12:263–73. - PubMed
-
- Aldinger G, De Pellegrin M, Kusswetter W. The personalized hip proshesis. Ital J Traumatol. 1988;14((4)):429–33. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous