

Mast cells and hypoxia drive tissue metaplasia and heterotopic ossification in idiopathic arthrofibrosis after total knee arthroplasty
- PMID: 20809936
- PMCID: PMC2940819
- DOI: 10.1186/1755-1536-3-17
Mast cells and hypoxia drive tissue metaplasia and heterotopic ossification in idiopathic arthrofibrosis after total knee arthroplasty
Abstract
Background: Idiopathic arthrofibrosis occurs in 3-4% of patients who undergo total knee arthroplasty (TKA). However, little is known about the cellular or molecular changes involved in the onset or progression of this condition. To classify the histomorphologic changes and evaluate potential contributing factors, periarticular tissues from the knees of patients with arthrofibrosis were analyzed for fibroblast and mast cell proliferation, heterotopic ossification, cellular apoptosis, hypoxia and oxidative stress.
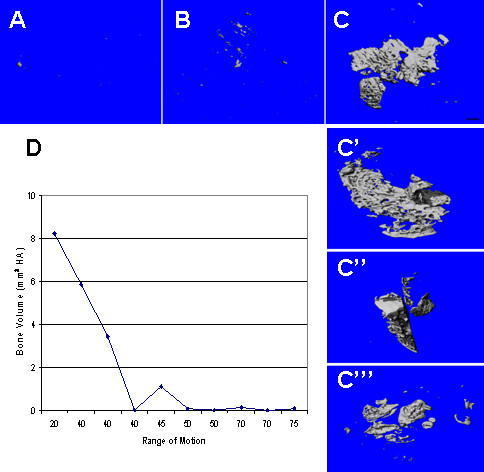
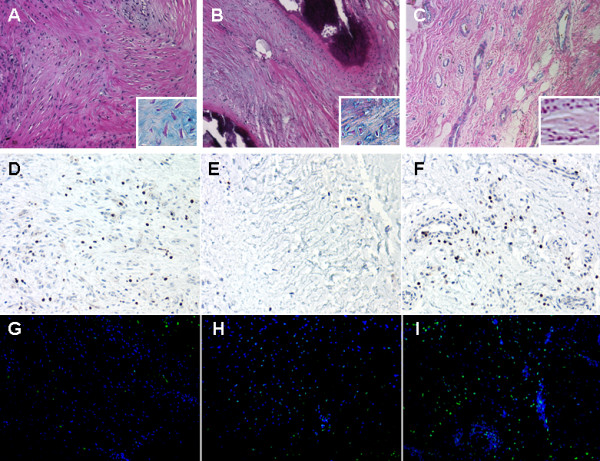
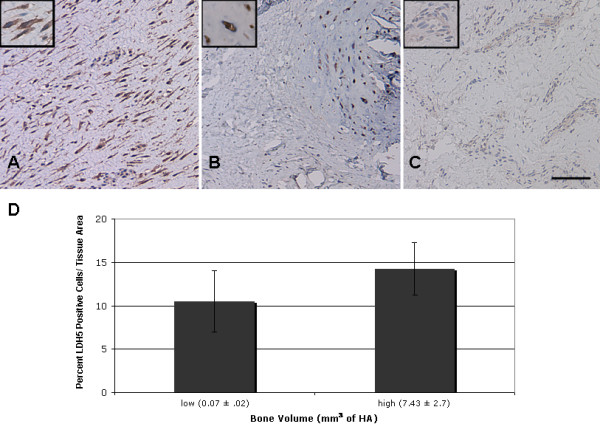
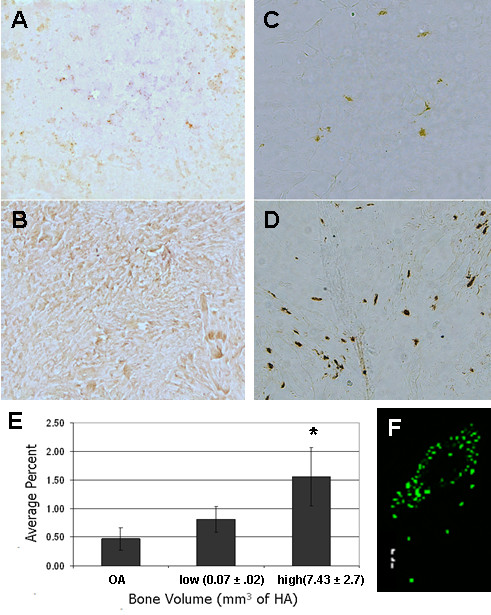
Results: The arthrofibrotic tissue was composed of dense fibroblastic regions, with limited vascularity along the outer edges. Within the fibrotic regions, elevated numbers of chymase/fibroblast growth factor (FGF)-expressing mast cells were observed. In addition, this region contained fibrocartilage and associated heterotopic ossification, which quantitatively correlated with decreased range of motion (stiffness). Fibrotic, fibrocartilage and ossified regions contained few terminal dUTP nick end labeling (TUNEL)-positive or apoptotic cells, despite positive immunostaining for lactate dehydrogenase (LDH)5, a marker of hypoxia, and nitrotyrosine, a marker for protein nitrosylation. LDH5 and nitrotyrosine were found in the same tissue areas, indicating that hypoxic areas within the tissue were associated with increased production of reactive oxygen and nitrogen species.
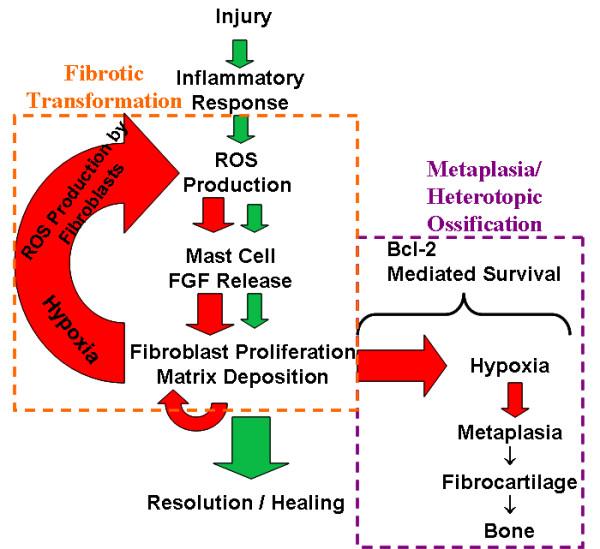
Conclusions: Taken together, we suggest that hypoxia-associated oxidative stress initiates mast cell proliferation and FGF secretion, spurring fibroblast proliferation and tissue fibrosis. Fibroblasts within this hypoxic environment undergo metaplastic transformation to fibrocartilage, followed by heterotopic ossification, resulting in increased joint stiffness. Thus, hypoxia and associated oxidative stress are potential therapeutic targets for fibrosis and metaplastic progression of idiopathic arthrofibrosis after TKA.
Figures
References
-
- Anouchi YS, McShane M, Kelly F, Elting J, Stiehl J. Range of motion in total knee replacement. Clinical Orthopaedics & Related Research. 1996;331:87–92. - PubMed
-
- Kim J, Nelson CL, Lotke PA. Stiffness after total knee arthroplasty. Prevalence of the complication and outcomes of revision. Journal of Bone & Joint Surgery American. 2004;86:1479–1484. - PubMed
-
- Mont MA, Serna FK, Krackow KA, Hungerford DS. Exploration of radiographically normal total knee replacements for unexplained pain. Clinical Orthopaedics & Related Research. 1996;331:216–220. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
