

MRS-guided HDR brachytherapy boost to the dominant intraprostatic lesion in high risk localised prostate cancer
- PMID: 20809986
- PMCID: PMC2941503
- DOI: 10.1186/1471-2407-10-472
MRS-guided HDR brachytherapy boost to the dominant intraprostatic lesion in high risk localised prostate cancer
Abstract
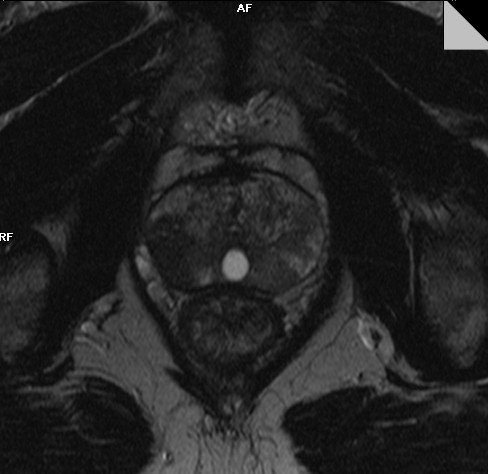
Background: It is known that the vast majority of prostate cancers are multifocal. However radical radiotherapy historically treats the whole gland rather than individual cancer foci.Magnetic resonance spectroscopy (MRS) can be used to non-invasively locate individual cancerous tumours in prostate. Thus an intentionally non-uniform dose distribution treating the dominant intraprostatic lesion to different dose levels than the remaining prostate can be delivered ensuring the maximum achievable tumour control probability.The aim of this study is to evaluate, using radiobiological means, the feasibility of a MRS-guided high dose rate (HDR) brachytherapy boost to the dominant lesion.
Methods: Computed tomography and MR/MRS were performed for treatment planning of a high risk localised prostate cancer. Both were done without endorectal coil, which distorts shape of prostate during the exams.Three treatment plans were compared:- external beam radiation therapy (EBRT) only- combination of EBRT and HDR brachytherapy- combination of EBRT and HDR brachytherapy with a synchronous integrated boost to the dominant lesionThe criteria of plan comparison were: the minimum, maximum and average doses to the targets and organs at risk; dose volume histograms; biologically effective doses for organs at risk and tumour control probability for the target volumes consisting of the dominant lesion as detected by MR/MRS and the remaining prostate volume.
Results: Inclusion of MRS information on the location of dominant lesion allows a safe increase of the dose to the dominant lesion while dose to the remaining target can be even substantially decreased keeping the same, high tumour control probability. At the same time an improved urethra sparing was achieved comparing to the treatment plan using a combination of EBRT and uniform HDR brachytherapy.
Conclusions: MRS-guided HDR brachytherapy boost to dominant lesion has the potential to spare the normal tissue, especially urethra, while keeping the tumour control probability high.
Figures



References
-
- Kurhanewicz J, Vigneron DB, Hricak H, Narayan P, Carroll P, Nelson SJ. Three-dimensional H-1 MR spectroscopic imaging of the in situ human prostate with high (0.24-0.7-cm3) spatial resolution. Radiology. 1996;198(3):795–805. - PubMed
-
- Kaji Y, Kurhanewicz J, Hricak H, Sokolov DL, Huang LR, Nelson SJ, Vigneron DB. Localizing prostate cancer in the presence of postbiopsy changes on MR images: role of proton MR spectroscopic imaging. Radiology. 1998;206(3):785–90. - PubMed
-
- Yu KK, Scheidler J, Hricak H, Vigneron DB, Zaloudek CJ, Males RG, Nelson SJ, Carroll PR, Kurhanewicz J. Prostate cancer: prediction of extracapsular extension with endorectal MR imaging and three-dimensional proton MR spectroscopic imaging. Radiology. 1999;213(2):481–8. - PubMed
-
- Pickett B, Kurhanewicz J, Coakley F, Shinohara K, Fein B, Roach M. Use of MRI and spectroscopy in evaluation of external beam radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2004;60(4):1047–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
