

Bone-to-bone fixation enhances functional healing of the porcine anterior cruciate ligament using a collagen-platelet composite
- PMID: 20810092
- PMCID: PMC2936961
- DOI: 10.1016/j.arthro.2009.12.017
Bone-to-bone fixation enhances functional healing of the porcine anterior cruciate ligament using a collagen-platelet composite
Abstract
Purpose: The purpose of this study was to determine whether providing bony stabilization between the tibia and femur improves the structural properties of an "enhanced" anterior cruciate ligament (ACL) repair using a collagen-platelet composite when compared with the traditional (Marshall) suture technique.
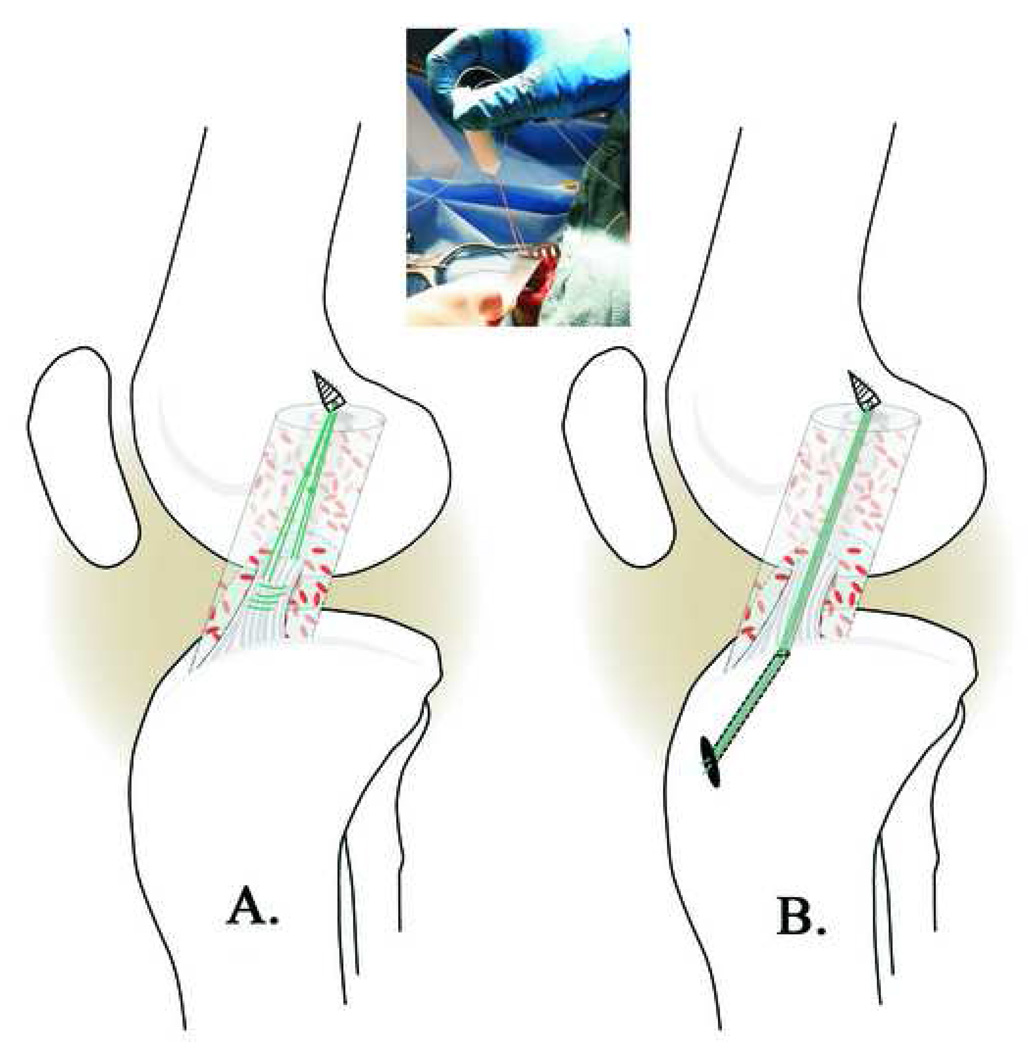
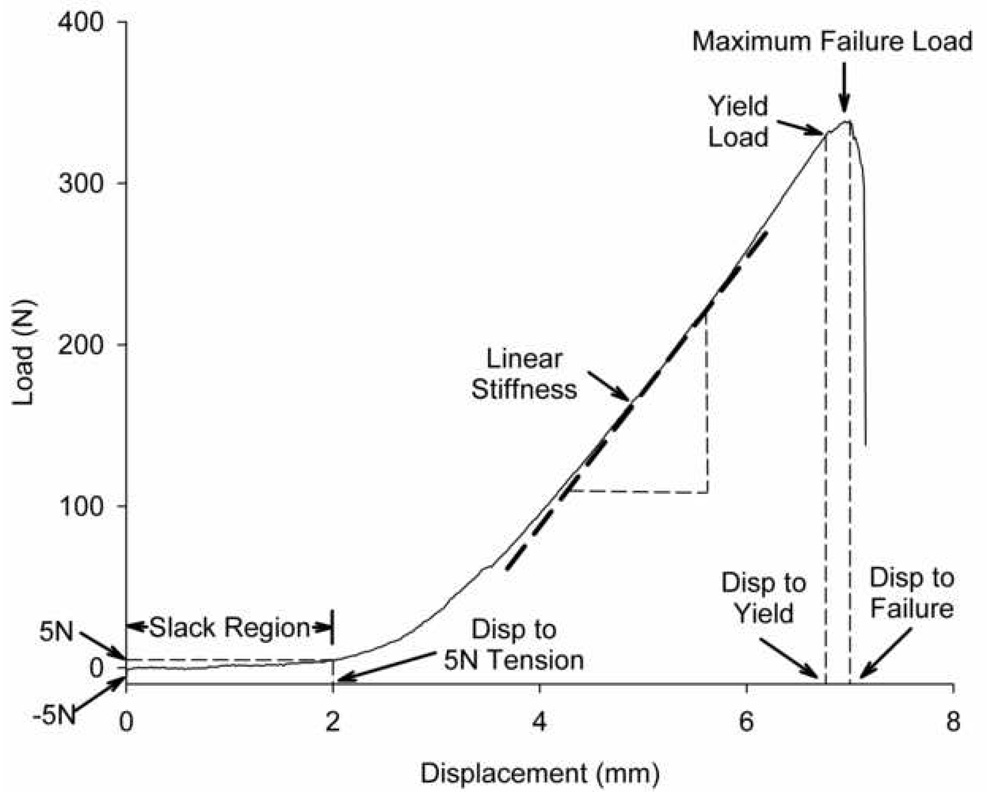
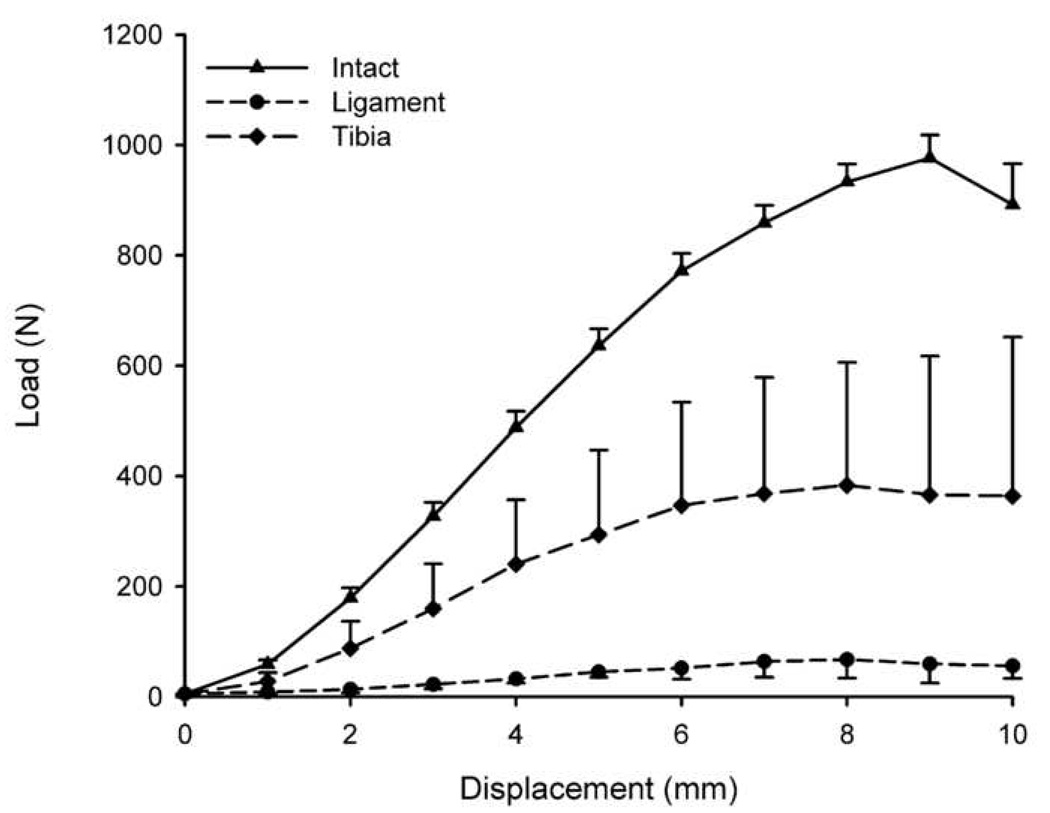
Methods: Twelve pigs underwent unilateral ACL transection and were treated with sutures connecting the bony femoral ACL attachment site to the distal ACL stump (ligament group) or to the tibia through a bone tunnel (tibia group). A collagen-platelet composite was placed around the sutures to enhance the biological repair in both groups. Anteroposterior knee laxity and the graft structural properties were measured after 15 weeks of healing in both the ACL-repaired and contralateral, ACL-intact joints.
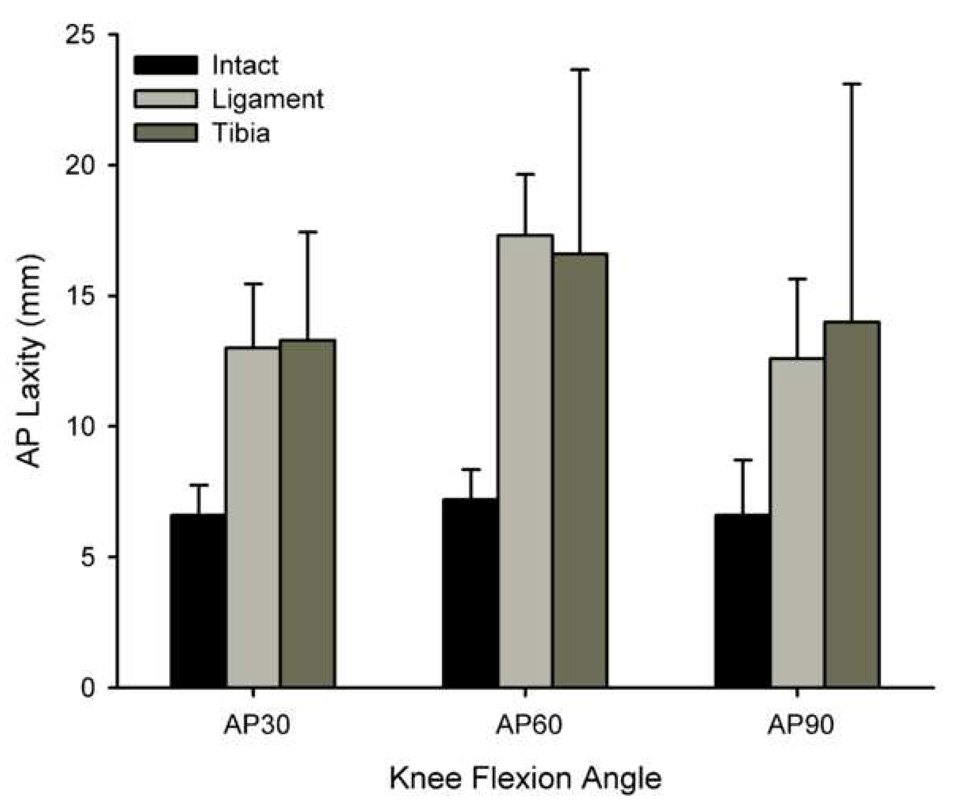
Results: Enhanced ACL repair with bone-to-bone fixation significantly improved yield load and linear stiffness of the ACL repairs (P < .05) after 15 weeks of healing. However, laxity values of the knees were similar in both groups of repaired knees (P > .10).
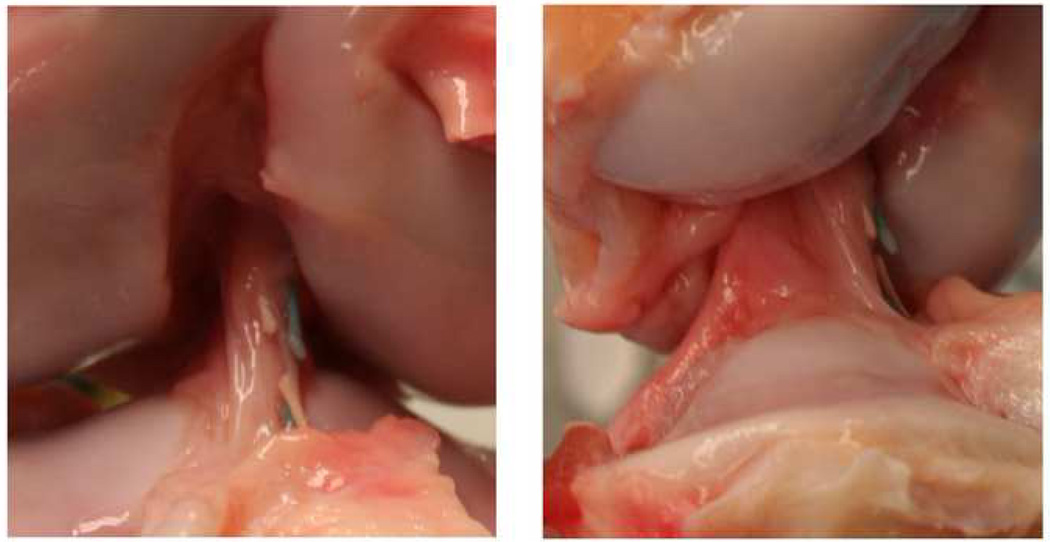
Conclusions: Using an enhanced ACL suture repair technique that includes bone-to-bone fixation to protect the repair in the initial healing stages resulted in an ACL with improved structural properties after 15 weeks in the porcine model.
Clinical relevance: The healing response of an ACL suture repair by use of a collagen-platelet composite can be enhanced by providing bony stabilization between the tibia and femur to protect the graft during the initial healing process in a translational model.
Figures
References
-
- Hefti FL, Kress I, Fasel J, Morscher EW. Healing of the transected anterior cruciate ligament in the rabbit. J Bone Joint Surg Am. 1991;73:373–383. - PubMed
-
- Cabaud HE, Rodkey WG, Feagin JA. Experimental studies of acute anterior cruciate ligament injury and repair. Am J Sports Med. 1979;7:18–22. - PubMed
-
- O'Donoghue DH, Frank GR, Jeter GL, Johnson W, Zeiders JW, Kenyon R. Repair and reconstruction of the anterior cruciate ligament in dogs. Factors influencing long-term results. J Bone Joint Surg Am. 1971;53:710–718. - PubMed
-
- O'Donoghue DH, Rockwood C, Frank GR, Jack SC, Kenyon R. Repair of the anterior cruciate ligament in dogs. J Bone Joint Surg Am. 1966;48:503–519. - PubMed
-
- Feagin JA, Curl WW. Isolated tear of the anterior cruciate ligament: 5-year follow-up study. Am J Sports Med. 1976;4:95–100. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
