

Probabilistic learning and inference in schizophrenia
- PMID: 20810252
- PMCID: PMC3008301
- DOI: 10.1016/j.schres.2010.08.009
Probabilistic learning and inference in schizophrenia
Abstract
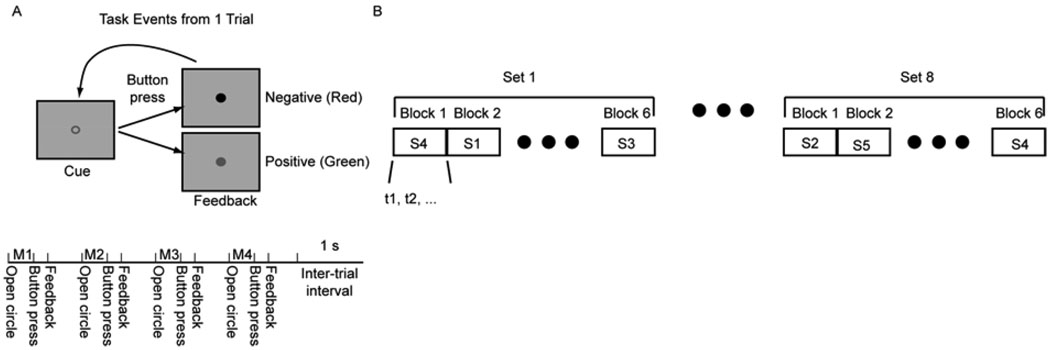
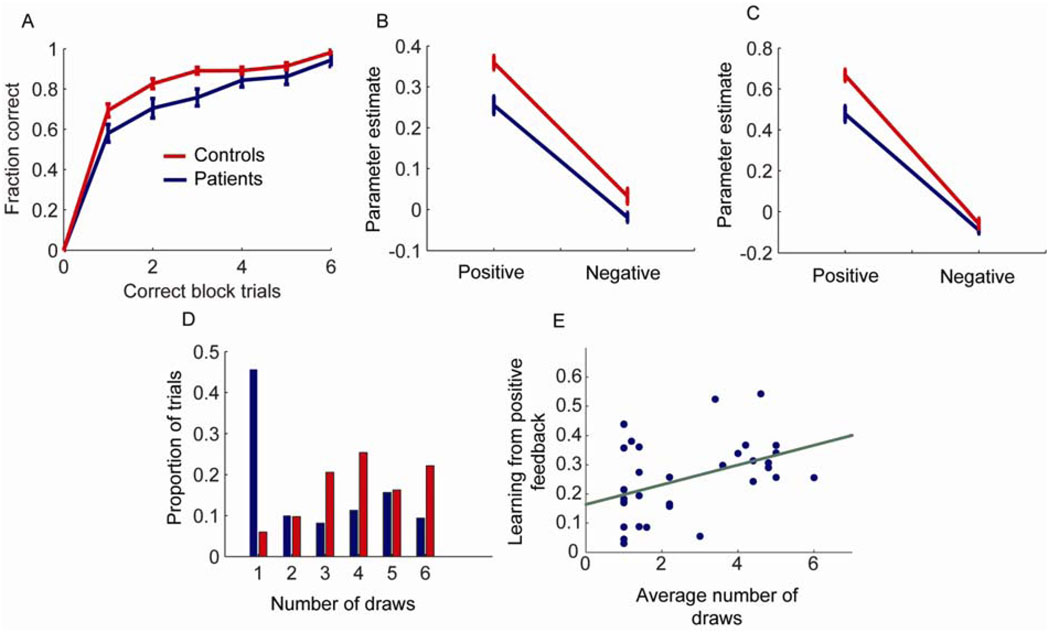
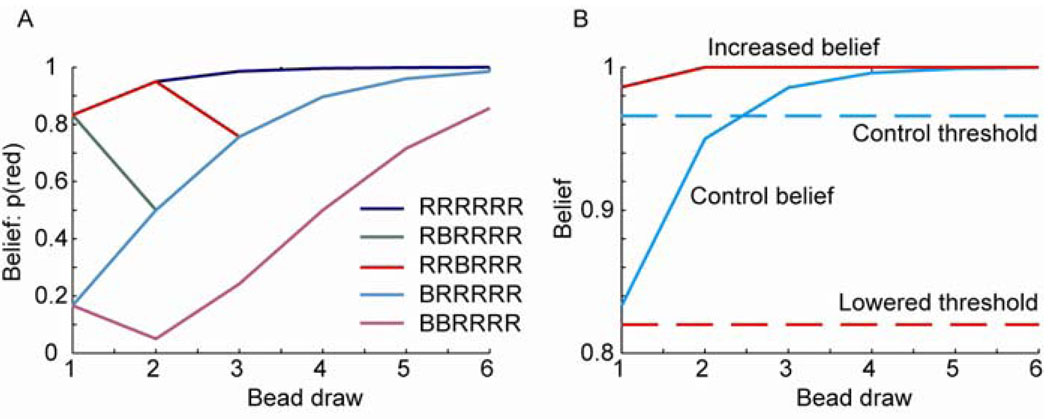
Patients with schizophrenia make decisions on the basis of less evidence when required to collect information to make an inference, a behavior often called jumping to conclusions. The underlying basis for this behavior remains controversial. We examined the cognitive processes underpinning this finding by testing subjects on the beads task, which has been used previously to elicit jumping to conclusions behavior, and a stochastic sequence learning task, with a similar decision theoretic structure. During the sequence learning task, subjects had to learn a sequence of button presses, while receiving a noisy feedback on their choices. We fit a Bayesian decision making model to the sequence task and compared model parameters to the choice behavior in the beads task in both patients and healthy subjects. We found that patients did show a jumping to conclusions style; and those who picked early in the beads task tended to learn less from positive feedback in the sequence task. This favours the likelihood of patients selecting early because they have a low threshold for making decisions, and that they make choices on the basis of relatively little evidence.
Published by Elsevier B.V.
Conflict of interest statement
Conflict of interest:
Over the last three years SSS has received study funding from Glaxo Smith Kline.
Figures
References
-
- Abi-Dargham A, Gil R, Krystal J, Baldwin RM, Seibyl JP, Bowers M, van Dyck CH, Charney DS, Innis RB, Laruelle M. Increased striatal dopamine transmission in schizophrenia: confirmation in a second cohort. Am J Psychiatry. 1998;155:761–767. - PubMed
-
- Breier A, Su TP, Saunders R, Carson RE, Kolachana BS, de Bartolomeis A, Weinberger DR, Weisenfeld N, Malhotra AK, Eckelman WC, Pickar D. Schizophrenia is associated with elevated amphetamine-induced synaptic dopamine concentrations: evidence from a novel positron emission tomography method. Proc Natl Acad Sci U S A. 1997;94:2569–2574. - PMC - PubMed
-
- Corcoran R, Rowse G, Moore R, Blackwood N, Kinderman P, Howard R, Cummins S, Bentall RP. A transdiagnostic investigation of 'theory of mind' and 'jumping to conclusions' in patients with persecutory delusions. Psychol Med. 2008;38:1577–1583. - PubMed
-
- Dudley RE, John CH, Young AW, Over DE. Normal and abnormal reasoning in people with delusions. Br J Clin Psychol. 1997;36(Pt 2):243–258. - PubMed
-
- Fine C, Gardner M, Craigie J, Gold I. Hopping, skipping or jumping to conclusions? Clarifying the role of the JTC bias in delusions. Cogn Neuropsychiatry. 2007;12:46–77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
