

Noncontact anterior cruciate ligament injuries: mechanisms and risk factors
- PMID: 20810933
- PMCID: PMC3625971
- DOI: 10.5435/00124635-201009000-00003
Noncontact anterior cruciate ligament injuries: mechanisms and risk factors
Abstract
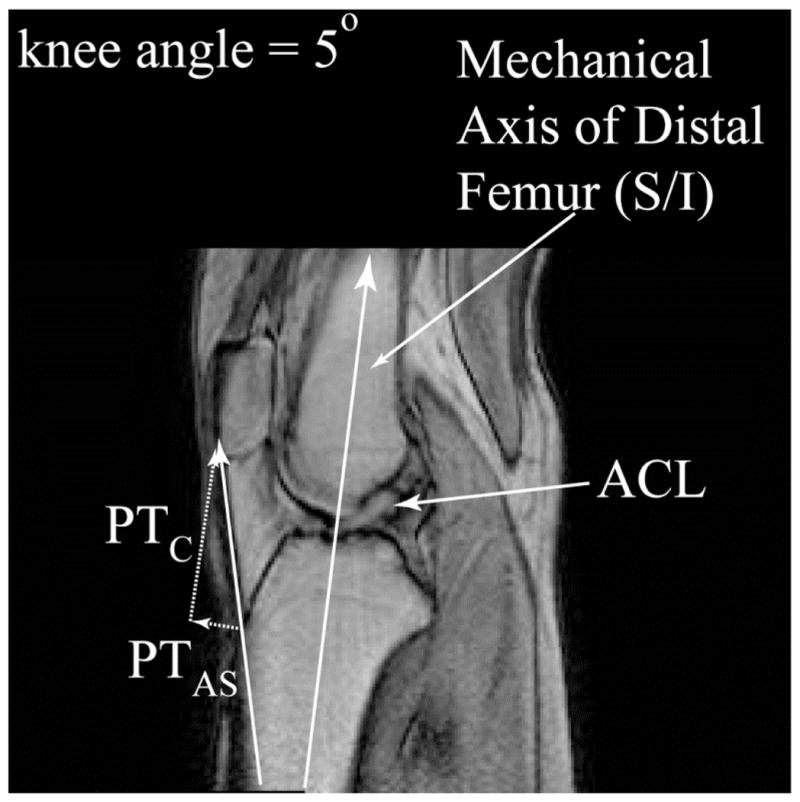
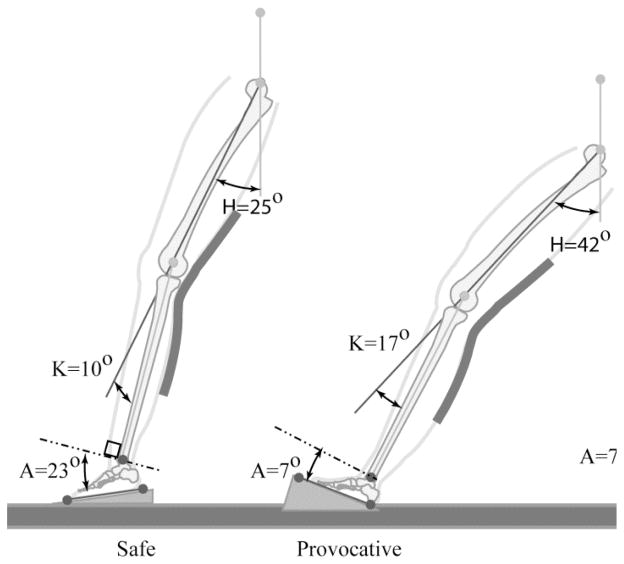
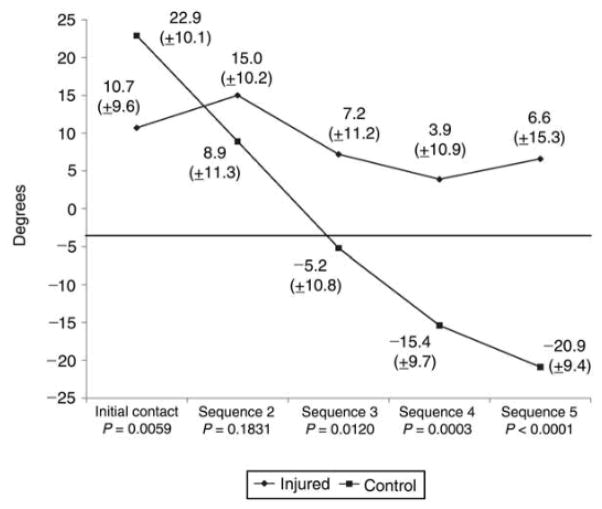
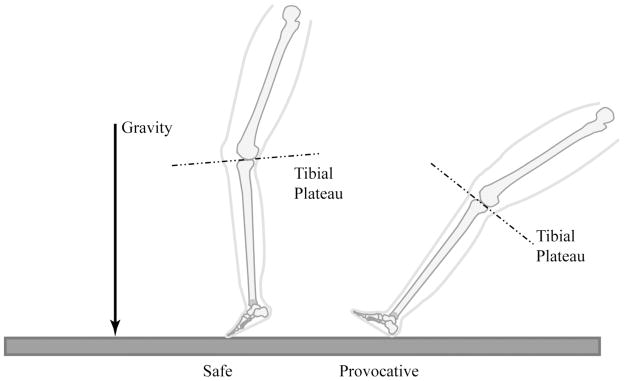
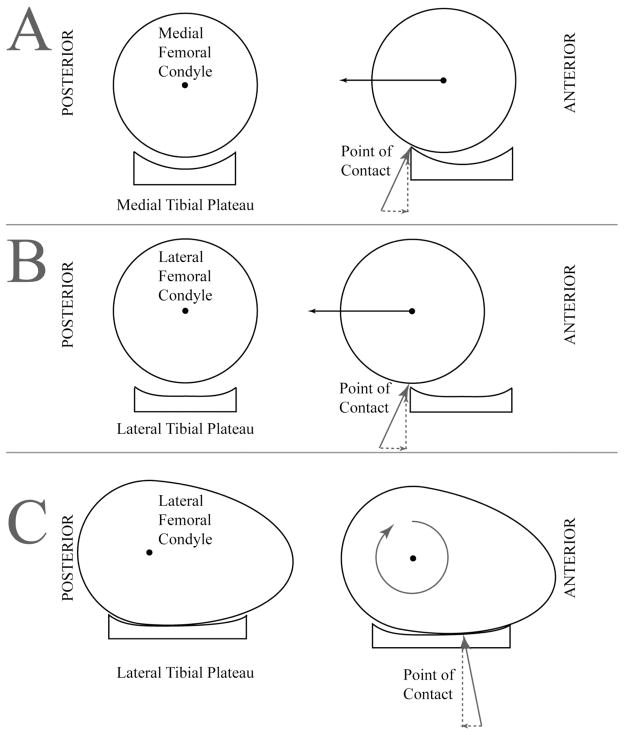
Significant advances have recently been made in understanding the mechanisms involved in noncontact anterior cruciate ligament (ACL) injury. Most ACL injuries involve minimal to no contact. Female athletes sustain a two- to eightfold greater rate of injury than do their male counterparts. Recent videotape analyses demonstrate significant differences in average leg and trunk positions during injury compared with control subjects. These findings as well as those of cadaveric and MRI studies indicate that axial compressive forces are a critical component in noncontact ACL injury. A complete understanding of the forces and risk factors associated with noncontact ACL injury should lead to the development of improved preventive strategies for this devastating injury.
Figures
References
-
- Boden BP, Dean GS, Feagin JA, Jr, Garrett WE., Jr Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23:573–578. - PubMed
-
- Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St PP, Taylor DC. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med. 2003;31:831–842. - PubMed
-
- DeMorat G, Weinhold P, Blackburn T, Chudik S, Garrett W. Aggressive quadriceps loading can induce noncontact anterior cruciate ligament injury. Am J Sports Med. 2004;32:477–483. - PubMed
-
- Meyer EG, Baumer TG, Slade JM, Smith WE, Haut RC. Tibiofemoral contact pressures and osteochondral microtrauma during anterior cruciate ligament rupture due to excessive compressive loading and internal torque of the human knee. Am J Sports Med. 2008;36:1966–1977. - PubMed
-
- Boden BP, Torg JS, Knowles SB, Hewett TE. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37:252–259. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
