

B cell subsets contribute to renal injury and renal protection after ischemia/reperfusion
- PMID: 20810984
- PMCID: PMC3133676
- DOI: 10.4049/jimmunol.0903239
B cell subsets contribute to renal injury and renal protection after ischemia/reperfusion
Abstract
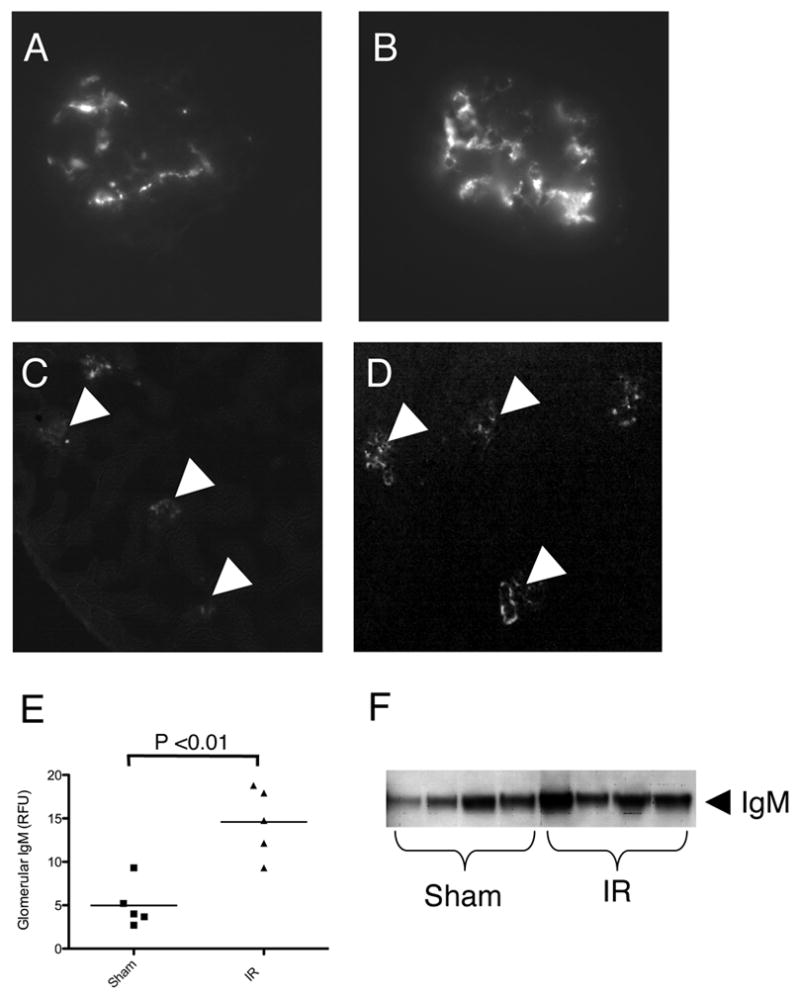
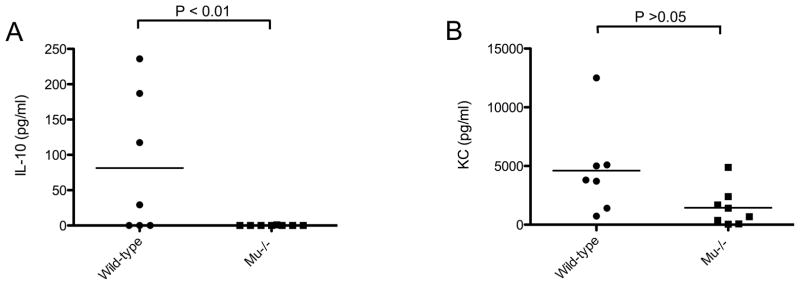
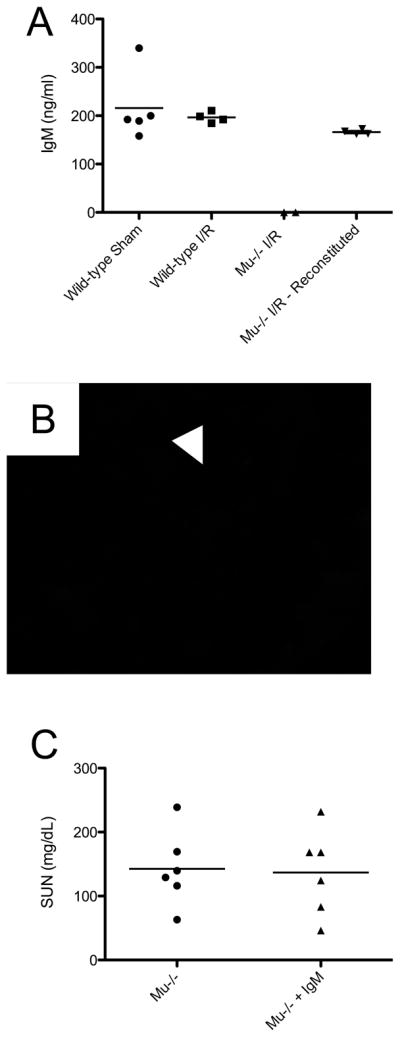
Ischemia/reperfusion (I/R) triggers a robust inflammatory response within the kidney. Numerous components of the immune system contribute to the resultant renal injury, including the complement system. We sought to identify whether natural Abs bind to the postischemic kidney and contribute to complement activation after I/R. We depleted peritoneal B cells in mice by hypotonic shock. Depletion of the peritoneal B cells prevented the deposition of IgM within the glomeruli after renal I/R and attenuated renal injury after I/R. We found that glomerular IgM activates the classical pathway of complement, but it does not cause substantial deposition of C3 within the kidney. Furthermore, mice deficient in classical pathway proteins were not protected from injury, indicating that glomerular IgM does not cause injury through activation of the classical pathway. We also subjected mice deficient in all mature B cells (μMT mice) to renal I/R and found that they sustained worse renal injury than wild-type controls. Serum IL-10 levels were lower in the μMT mice. Taken together, these results indicate that natural Ab produced by peritoneal B cells binds within the glomerulus after renal I/R and contributes to functional renal injury. However, nonperitoneal B cells attenuate renal injury after I/R, possibly through the production of IL-10.
Figures





References
-
- Bonventre JV, Zuk A. Ischemic acute renal failure: An inflammatory disease? Kidney Int. 2004;66:480–485. - PubMed
-
- Thurman JM, Ljubanovic D, Edelstein CL, Gilkeson GS, Holers VM. Lack of a functional alternative complement pathway ameliorates ischemic acute renal failure in mice. J Immunol. 2003;170:1517–1523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
