

Treatment of common congenital hand conditions
- PMID: 20811188
- PMCID: PMC4404786
- DOI: 10.1097/PRS.0b013e3181e605be
Treatment of common congenital hand conditions
Abstract
Learning objectives: After reading this article, the participant should be able to: 1. Recognize the clinical features associated with five common congenital hand conditions. 2. Describe the indications and appropriate timing for various surgical procedures used to treat congenital hand anomalies. 3. Identify the pearls and pitfalls of these surgical treatments to avoid complications. 4. Understand the expected postoperative outcomes associated with these surgical procedures.
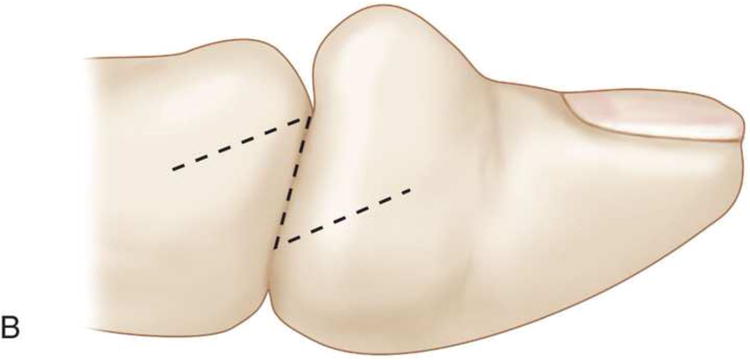
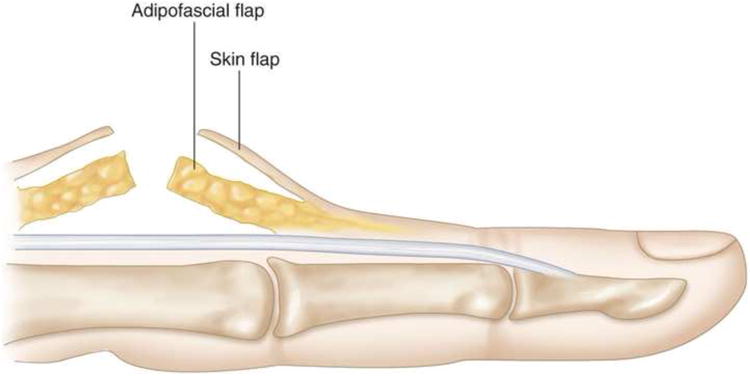
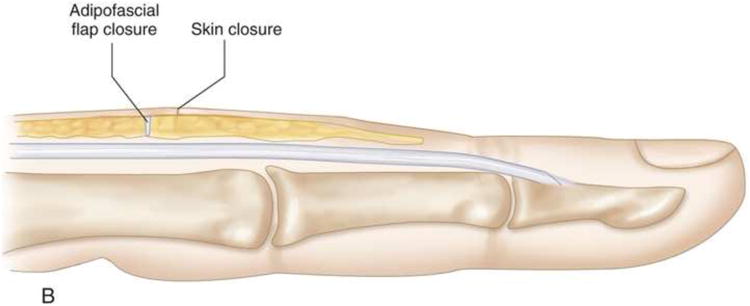
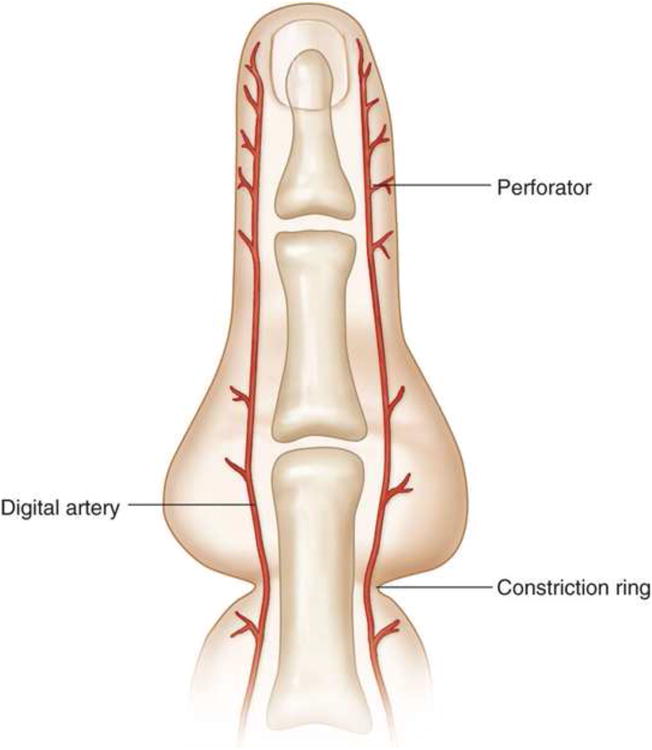
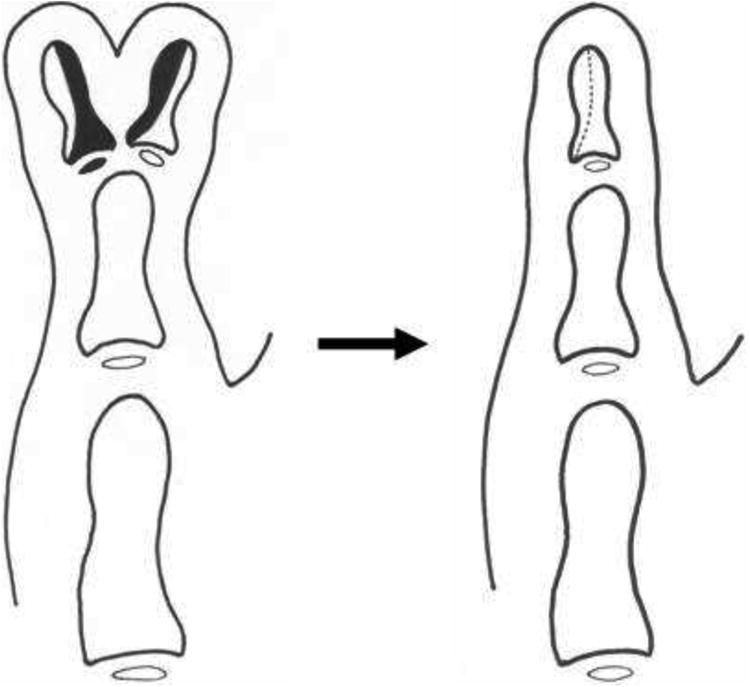
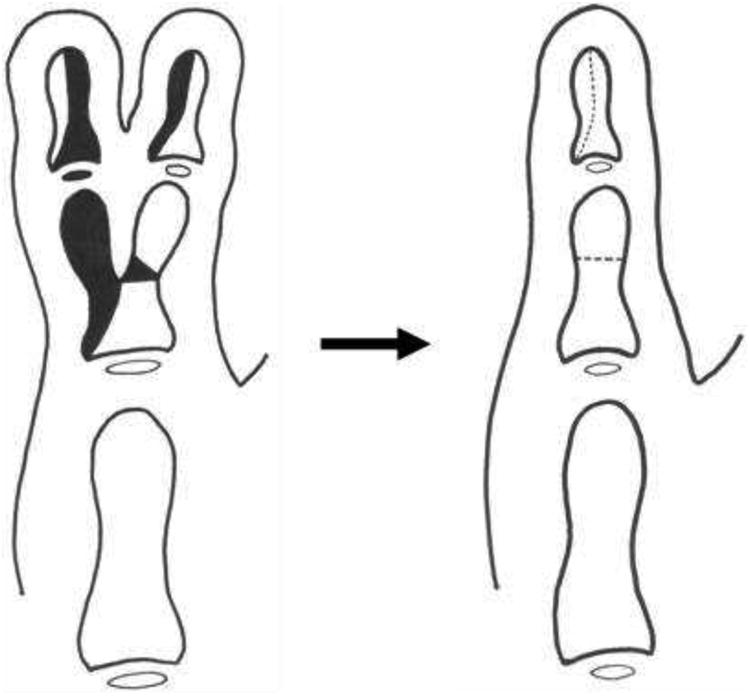
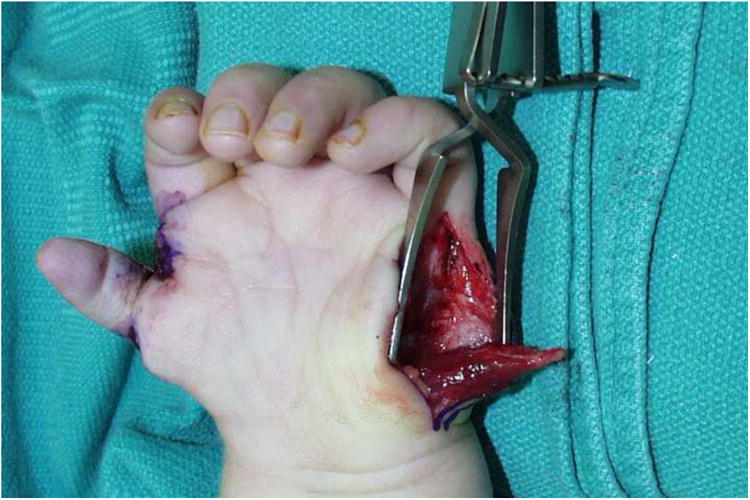
Summary: This article provides an introduction to congenital hand differences by focusing on practical surgical strategies for treating five commonly encountered conditions, including syndactyly, constriction ring syndrome, duplicated thumb, hypoplastic thumb, and trigger thumb. The accompanying videos demonstrate common and reliable surgical techniques for syndactyly release, duplicated thumb reconstruction, and pollicization for hypoplastic thumb.
Figures










Similar articles
-
Congenital Anomalies of the Hand--Principles of Management.Orthop Clin North Am. 2016 Jan;47(1):153-68. doi: 10.1016/j.ocl.2015.08.015. Orthop Clin North Am. 2016. PMID: 26614930 Review.
-
Common Pediatric Congenital Conditions of the Hand.Plast Reconstr Surg. 2015 Aug;136(2):241e-257e. doi: 10.1097/PRS.0000000000001499. Plast Reconstr Surg. 2015. PMID: 26218399 Review.
-
Pollicization: the concept, technical details, and outcome.Clin Orthop Surg. 2012 Mar;4(1):18-35. doi: 10.4055/cios.2012.4.1.18. Epub 2012 Feb 20. Clin Orthop Surg. 2012. PMID: 22379553 Free PMC article. Review.
-
Polydactyly of the Hand.J Am Acad Orthop Surg. 2018 Feb 1;26(3):75-82. doi: 10.5435/JAAOS-D-16-00139. J Am Acad Orthop Surg. 2018. PMID: 29309292 Review.
-
Long-finger pollicization for macrodactyly of the thumb and index finger.J Pediatr Orthop. 2014 Oct-Nov;34(7):e50-3. doi: 10.1097/BPO.0000000000000232. J Pediatr Orthop. 2014. PMID: 24919138
Cited by
-
Radiographic indicators of a shared epiphysis in radial polydactyly.Hand (N Y). 2014 Sep;9(3):329-34. doi: 10.1007/s11552-013-9593-7. Hand (N Y). 2014. PMID: 25191163 Free PMC article.
-
Syndactyly Release.Semin Plast Surg. 2016 Nov;30(4):162-170. doi: 10.1055/s-0036-1593478. Semin Plast Surg. 2016. PMID: 27895538 Free PMC article. Review.
-
New Simple Technique for Syndactyly Release.Plast Reconstr Surg Glob Open. 2020 May 14;8(5):e2842. doi: 10.1097/GOX.0000000000002842. eCollection 2020 May. Plast Reconstr Surg Glob Open. 2020. PMID: 33133902 Free PMC article.
-
Using Dermal Fat Graft to Release Complex Syndactyly: A New Method.Plast Reconstr Surg Glob Open. 2020 Aug 17;8(8):e3068. doi: 10.1097/GOX.0000000000003068. eCollection 2020 Aug. Plast Reconstr Surg Glob Open. 2020. PMID: 32983810 Free PMC article. No abstract available.
-
The Impact of Microsurgery on Congenital Hand Anomalies Associated with Amniotic Band Syndrome.Plast Reconstr Surg Glob Open. 2018 Apr 4;6(4):e1657. doi: 10.1097/GOX.0000000000001657. eCollection 2018 Apr. Plast Reconstr Surg Glob Open. 2018. PMID: 29876159 Free PMC article.
References
-
- Tonkin MA. Failure of Differentiation Part 1: Syndactyly. Hand Clin. 2009;25(2):171–193. - PubMed
-
- Kozin SH. Syndactyly. J Am Soc Surg Hand. 2001;1:1–13.
-
- Flatt AE. Practical factors in the treatment of syndactyly. In: Littler JW, Cramer LM, Smith JW, editors. Symposium on reconstructive hand surgery. Vol. 9. St. Louis: CV Mosby; 1974. pp. 144–156.
-
- Kim SE, Chung KC. Syndacty release. In: Chung KC, editor. Operative technique; hand and wrist surgery. Vol. 2. Philadelphia: Saunders Elsevier; 2008. pp. 847–858.
-
- Kay SP. Syndactyly. In: Green DP, Pederson WC, Hotchkiss RN, et al., editors. Green's operative hand surgery. 5. Vol. 2. Philadelphia: Elsevier Churchi Livingstone; 2005. pp. 1381–1393.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
