

Premature Ventricular Contractions and Non-sustained Ventricular Tachycardia: Association with Sudden Cardiac Death, Risk Stratification, and Management Strategies
- PMID: 20811538
- PMCID: PMC2922873
Premature Ventricular Contractions and Non-sustained Ventricular Tachycardia: Association with Sudden Cardiac Death, Risk Stratification, and Management Strategies
Abstract
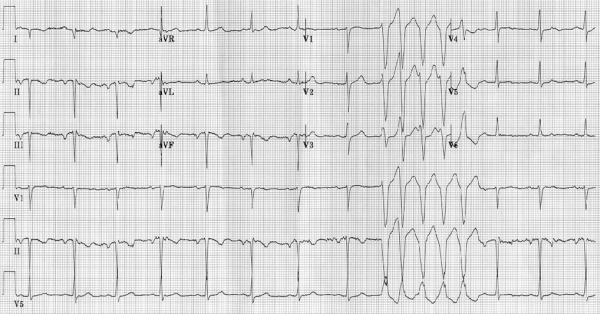
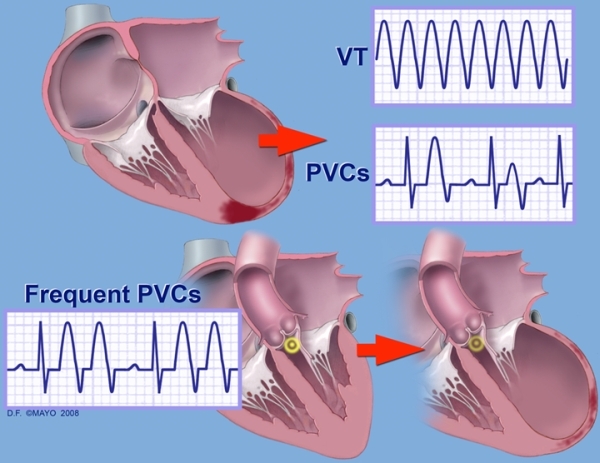
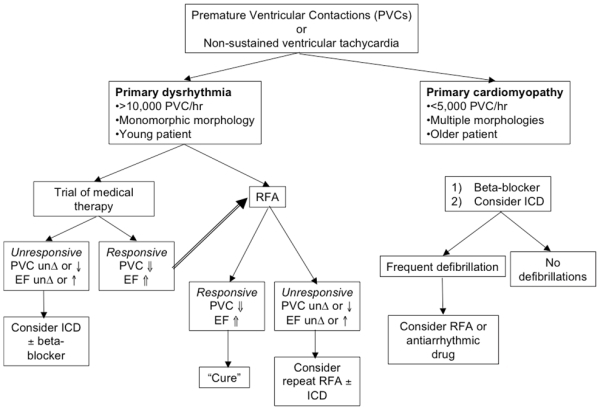
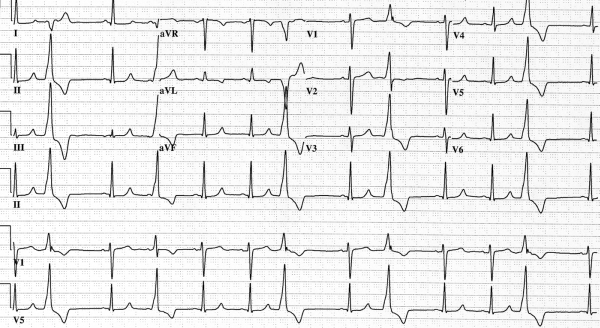
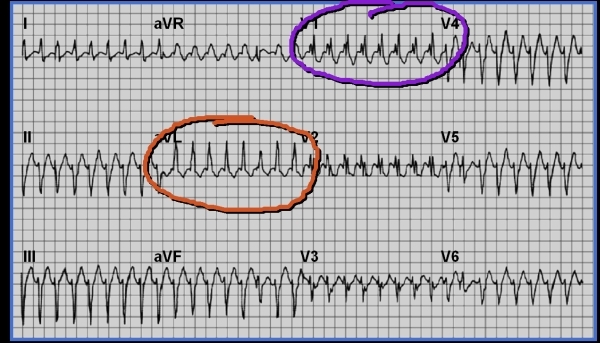
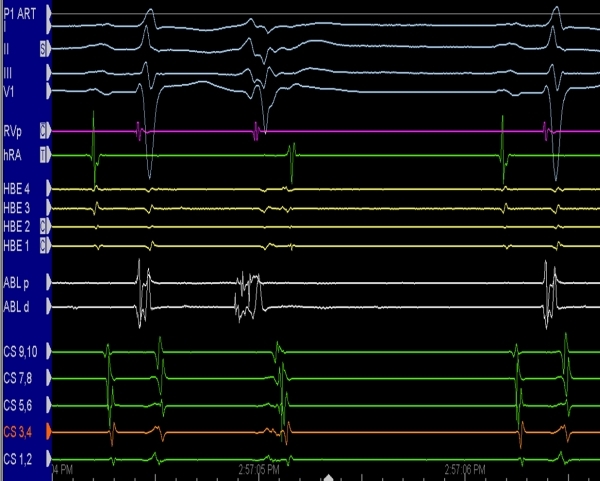
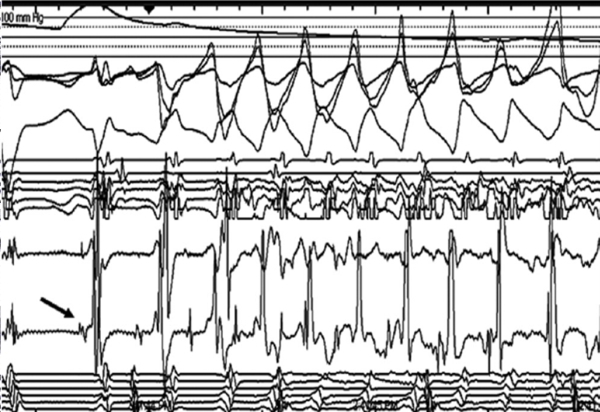
Premature ventricular contractions (PVCs) and non-sustained ventricular tachycardia (NSVT) are frequently encountered and a marker of electrocardiomyopathy. In some instances, they increase the risk for sustained ventricular tachycardia, ventricular fibrillation, and sudden cardiac death. While often associated with a primary cardiomyopathy, they have also been known to cause tachycardia-induced cardiomyopathy in patients without preceding structural heart disease. Medical therapy including beta-blockers and class III anti-arrhythmic agents can be effective while implantable cardiac defibrillators (ICD) are indicated in certain patients. Radiofrequency ablation (RFA) is the preferred, definitive treatment in those patients that improve with anti-arrhythmic therapy, have tachycardia-induced cardiomyopathy, or have certain subtypes of PVCs/NSVT. We present a review of PVCs and NSVT coupled with case presentations on RFA of fascicular ventricular tachycardia, left-ventricular outflow tract ventricular tachycardia, and Purkinje arrhythmia leading to polymorphic ventricular tachycardia.
Keywords: PVC; ablation; premature ventricular contractions; sudden death; ventricular tachycardia.
Figures

Similar articles
-
Searching for a Solution: A Case Report on Multifocal Ectopic Purkinje-Related Premature Contractions Syndrome.Medicina (Kaunas). 2025 Feb 24;61(3):393. doi: 10.3390/medicina61030393. Medicina (Kaunas). 2025. PMID: 40142204 Free PMC article.
-
Current Concepts of Premature Ventricular Contractions.J Lifestyle Med. 2013 Mar;3(1):26-33. Epub 2013 Mar 31. J Lifestyle Med. 2013. PMID: 26064834 Free PMC article. Review.
-
Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: a single-center retrospective study.Heart Rhythm. 2014 Feb;11(2):187-93. doi: 10.1016/j.hrthm.2013.10.033. Epub 2013 Oct 22. Heart Rhythm. 2014. PMID: 24157533
-
Prognostic implications of premature ventricular contractions and non-sustained ventricular tachycardia in light-chain cardiac amyloidosis.Europace. 2024 Mar 1;26(3):euae063. doi: 10.1093/europace/euae063. Europace. 2024. PMID: 38466042 Free PMC article.
-
Role of antiarrhythmic therapy in patients at risk for sudden cardiac death: an evidence-based review.Pharmacotherapy. 2001 May;21(5):556-75. doi: 10.1592/phco.21.6.556.34550. Pharmacotherapy. 2001. PMID: 11349745 Review.
Cited by
-
Long-Term Outcome of Non-Sustained Ventricular Tachycardia in Structurally Normal Hearts.PLoS One. 2016 Aug 22;11(8):e0160181. doi: 10.1371/journal.pone.0160181. eCollection 2016. PLoS One. 2016. PMID: 27548469 Free PMC article.
-
Intramural anterolateral mitral annular idiopathic ventricular tachycardia successfully ablated from the atrium.HeartRhythm Case Rep. 2019 Apr 25;5(7):384-387. doi: 10.1016/j.hrcr.2019.04.002. eCollection 2019 Jul. HeartRhythm Case Rep. 2019. PMID: 31341783 Free PMC article. No abstract available.
-
From Incidental, Mechanically-Induced Arrhythmias to Reflex-Defined Arrhythmogenicity: On The Track of The Ternary Reflex System Resemblance to The "Infancy" of New Era or Rediscovery.J Atr Fibrillation. 2016 Feb 29;8(5):1377. doi: 10.4022/jafib.1377. eCollection 2016 Feb-Mar. J Atr Fibrillation. 2016. PMID: 27909483 Free PMC article. Review.
-
Association of premature ventricular complexes and risk of ischemic stroke: A systematic review and meta-analysis.Clin Cardiol. 2021 Feb;44(2):151-159. doi: 10.1002/clc.23531. Epub 2020 Dec 16. Clin Cardiol. 2021. PMID: 33325557 Free PMC article.
-
Clinical and Echocardiographic Predictors of Arrhythmias Detected With 24-Hour Holter Electrocardiography Among Hypertensive Heart Failure Patients in Nigeria.Clin Med Insights Cardiol. 2017 Dec 10;11:1179546817746632. doi: 10.1177/1179546817746632. eCollection 2017. Clin Med Insights Cardiol. 2017. PMID: 29270037 Free PMC article.
References
-
- Association AH. Dallas, Texas: 2010. Heart Disease and Stroke Statistics - 2010 Update.
-
- Myerburg RJ, et al. Sudden cardiac death: epidemiology, transient risk, and intervention assessment. Ann Intern Med. 1993;119:1187. - PubMed
-
- Fox CS, et al. Temporal trends in coronary heart disease mortality and sudden cardiac death from 1950 to 1999: the Framingham Heart Study. Circulation. 2004;110:522. - PubMed
-
- Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549. - PubMed
-
- Bernard S, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557. - PubMed
LinkOut - more resources
Full Text Sources