

Diagnosis and management of oropharyngeal Dysphagia and its nutritional and respiratory complications in the elderly
- PMID: 20811545
- PMCID: PMC2929516
- DOI: 10.1155/2011/818979
Diagnosis and management of oropharyngeal Dysphagia and its nutritional and respiratory complications in the elderly
Abstract
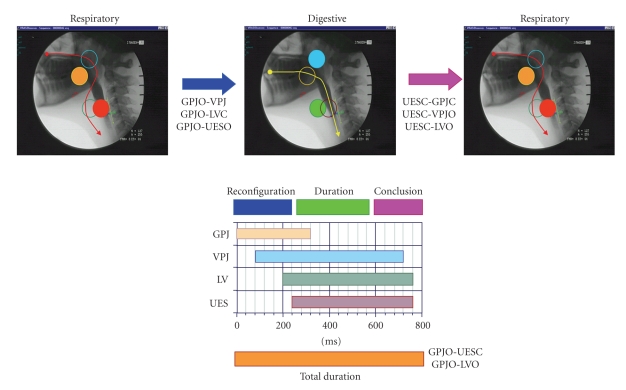
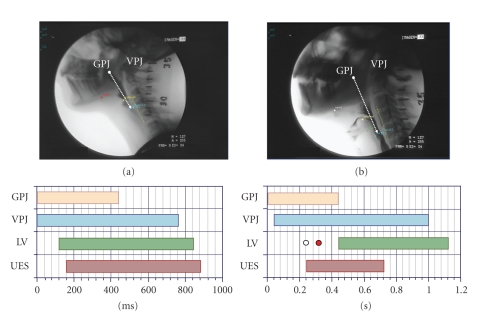
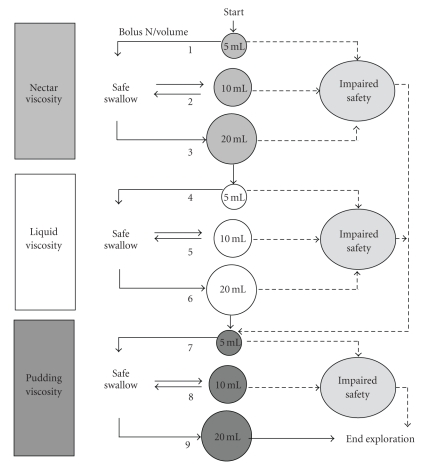
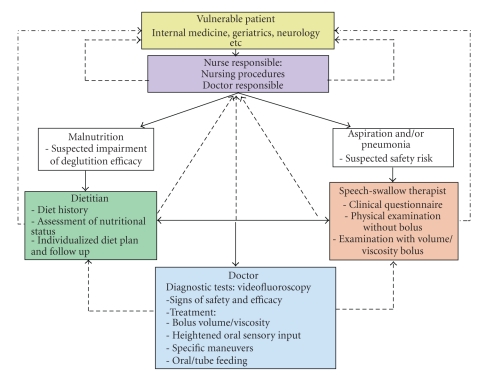
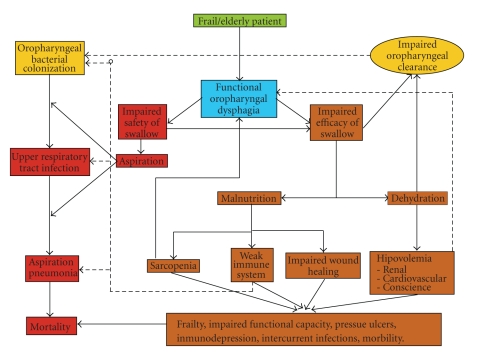
Oropharyngeal dysphagia is a major complaint among older people. Dysphagia may cause two types of complications in these patients: (a) a decrease in the efficacy of deglutition leading to malnutrition and dehydration, (b) a decrease in deglutition safety, leading to tracheobronchial aspiration which results in aspiration pneumonia and can lead to death. Clinical screening methods should be used to identify older people with oropharyngeal dysphagia and to identify those patients who are at risk of aspiration. Videofluoroscopy (VFS) is the gold standard to study the oral and pharyngeal mechanisms of dysphagia in older patients. Up to 30% of older patients with dysphagia present aspiration-half of them without cough, and 45%, oropharyngeal residue; and 55% older patients with dysphagia are at risk of malnutrition. Treatment with dietetic changes in bolus volume and viscosity, as well as rehabilitation procedures can improve deglutition and prevent nutritional and respiratory complications in older patients. Diagnosis and management of oropharyngeal dysphagia need a multidisciplinary approach.
Figures
References
-
- Clavé P, Verdaguer A, Arreola V. Oral-pharyngeal dysphagia in the elderly. Medicina Clinica. 2005;124(19):742–748. - PubMed
-
- Clavé P, Terré R, de Kraa M, Serra M. Approaching oropharyngeal dysphagia. Revista Espanola de Enfermedades Digestivas. 2004;96(2):119–131. - PubMed
-
- Ekberg O, Hamdy S, Woisard V, Wuttge-Hannig A, Ortega P. Social and psychological burden of dysphagia: its impact on diagnosis and treatment. Dysphagia. 2002;17(2):139–146. - PubMed
-
- Robbins J, Langmore S, Hind JA, Erlichman M. Dysphagia research in the 21st century and beyond: proceedings from Dysphagia Experts Meeting, August 21, 2001. Journal of Rehabilitation Research and Development. 2002;39(4):543–547. - PubMed
-
- Flacker JM. What is a geriatric syndrome anyway? Journal of the American Geriatrics Society. 2003;51(4):574–576. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
