Medullary carcinoma of the large intestine: a population based analysis
- PMID: 20811712
- PMCID: PMC4127912
- DOI: 10.3892/ijo_00000741
Medullary carcinoma of the large intestine: a population based analysis
Abstract
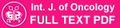
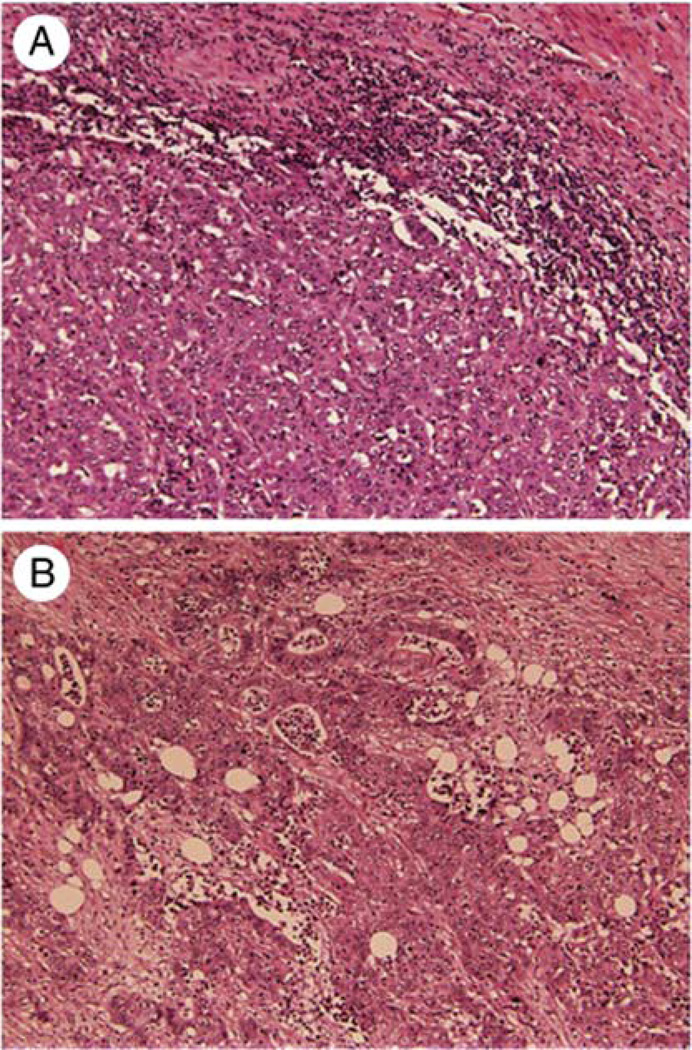
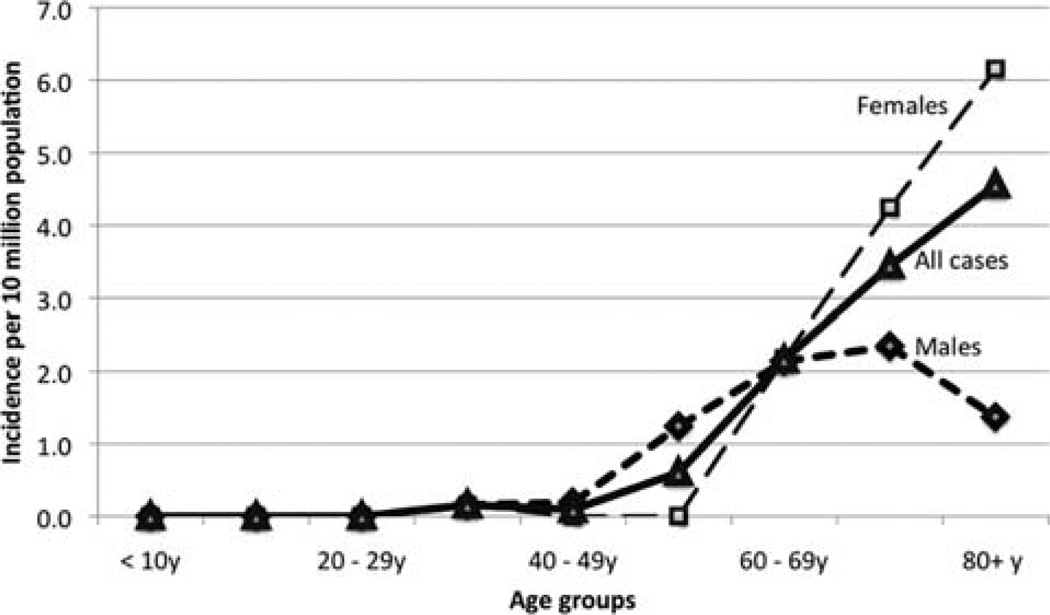
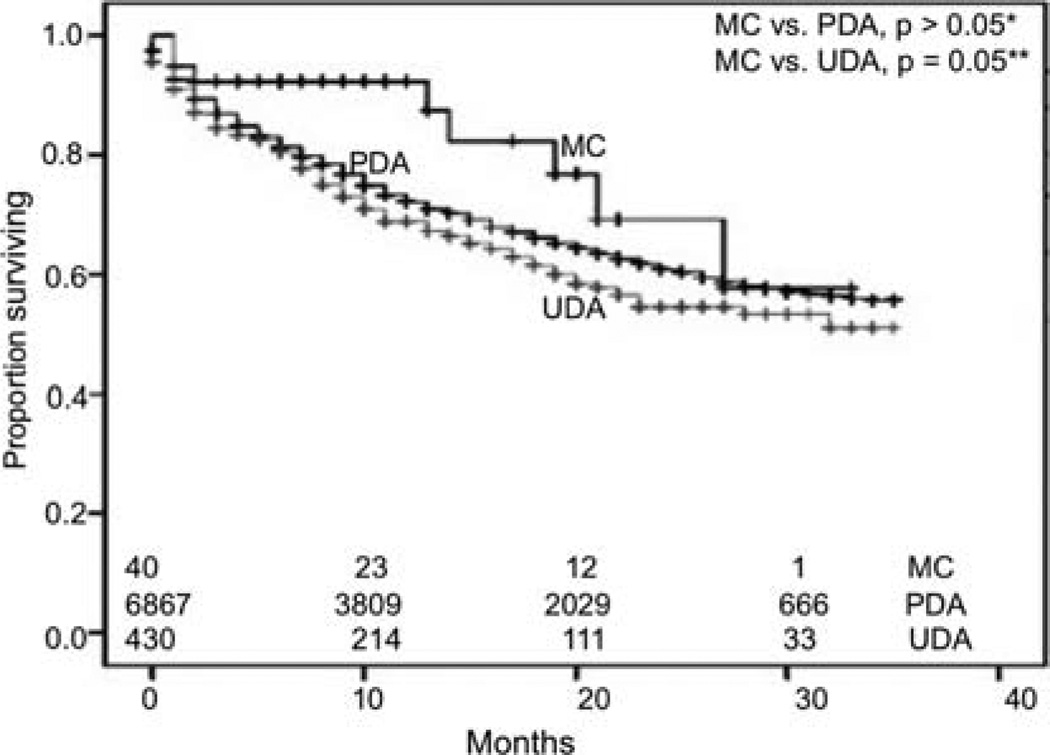
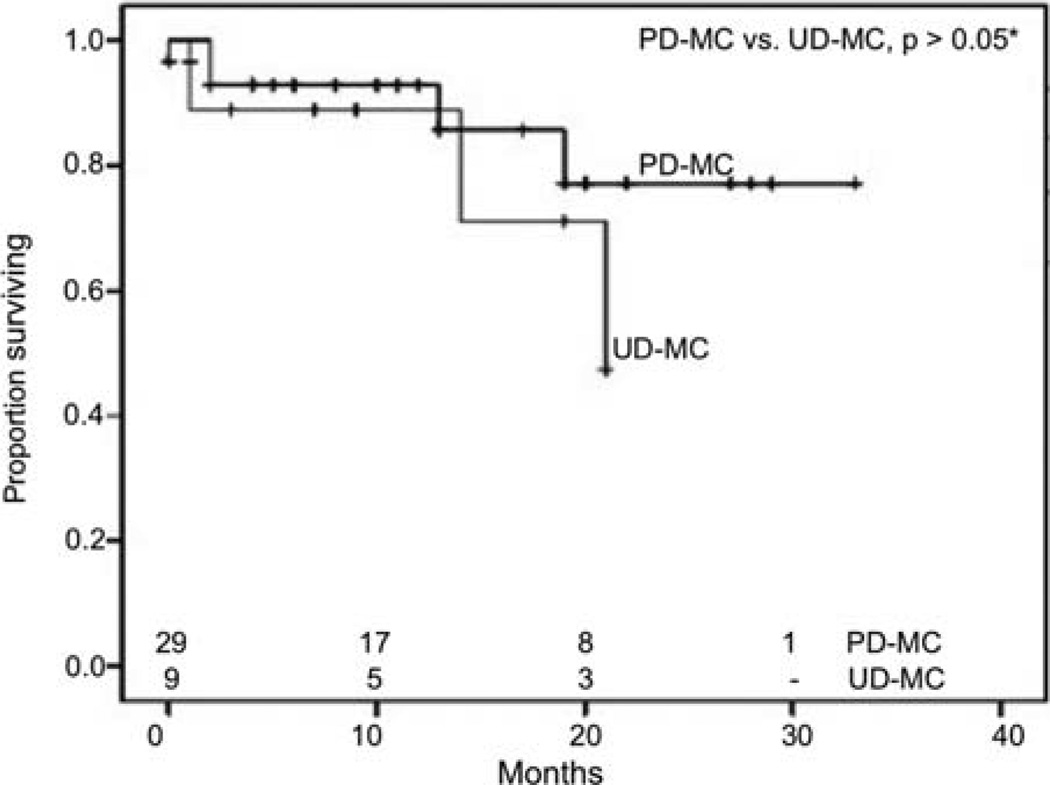
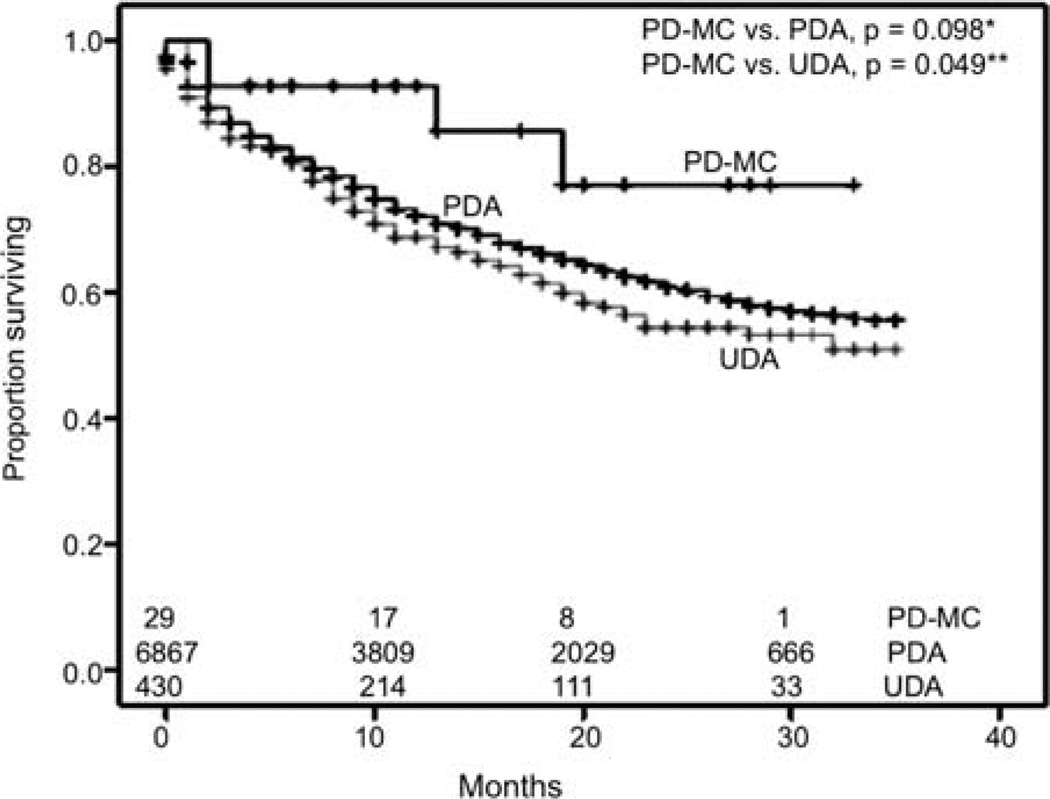
Medullary carcinoma (MC) of the colorectum is a relatively new histological type of adenocarcinoma characterized by poor glandular differentiation and intraepithelial lymphocytic infiltrate. To date, there has been no epidemiological study of this rare tumor type, which has now been incorporated as a separate entity in the World Health Organization (WHO) classification of colorectal cancers. We used the population-based registries of the Surveillance, Epidemiology and End Results (SEER) database to identify all cases of colorectal MC between 1973 and 2006 and compared them to poorly and undifferentiated colonic adenocarcinomas (PDA and UDA, respectively). We observed that MCs were rare tumors, constituting approximately 5-8 cases for every 10,000 colon cancers diagnosed, with a mean annual incidence of 3.47 (+/-0.75) per 10 million population. Mean age at diagnosis was 69.3 (+/-12.5) years, with incidence increasing with age. MCs were twice as common in females, who presented at a later age, with a lower stage and a trend towards favorable prognosis. MCs were extremely rare among African-Americans. MCs were most common in the proximal colon (74%), where they present at a later age than the sigmoid colon. There were no cases reliably identified in the rectum or appendix. Serum carcinoembryonic antigen levels (CEA) were elevated prior to first course of treatment in 40% of the patients. MCs were more commonly poorly differentiated (72%), with 22% being undifferentiated. MCs commonly presented with Stage II disease, with 10% presenting with metastases. Only one patient presented with N2b disease (>7 positive nodes). Early outcome analyses showed that MCs have 1- and 2-year relative survival rates of 92.7 and 73.8% respectively. Although MCs showed a trend towards better early overall survival, undifferentiated MCs present more commonly with Stage III, with comparatively worse early outcomes.
Figures
References
-
- Wick MR, Vitsky JL, Ritter JH, Swanson PE, Mills SE. Sporadic medullary carcinoma of the colon: a clinicopathologic comparison with nonhereditary poorly differentiated enteric-type adenocarcinoma and neuroendocrine colorectal carcinoma. Am J Clin Pathol. 2005;123:56–65. - PubMed
-
- Hamilton SR, Aaltonen LA, editors. World Health Organization Classification of Tumors. Lyon: IARC press; 2000. Pathology and genetics of tumors of the digestive system.
-
- Lanza G, Gafa R, Matteuzzi M, Santini A. Medullary-type poorly differentiated adenocarcinoma of the large bowel: a distinct clinicopathologic entity characterized by microsatellite instability and improved survival. J Clin Oncol. 1999;17:2429–2438. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical