

Standardization of surgical and pathologic variables is needed in multicenter trials of adjuvant therapy for pancreatic cancer: results from the ACOSOG Z5031 trial
- PMID: 20811779
- PMCID: PMC3922125
- DOI: 10.1245/s10434-010-1282-y
Standardization of surgical and pathologic variables is needed in multicenter trials of adjuvant therapy for pancreatic cancer: results from the ACOSOG Z5031 trial
Abstract
Background: Standardization of surgical and pathologic techniques is crucial to the interpretation of studies evaluating adjuvant therapies for pancreatic cancer (PC).
Methods: To assess the degree to which treatment administered prior to enrollment of patients in trials of adjuvant therapy is quality controlled, the operative and pathology reports of patients in American College of Surgeons Oncology Group (ACOSOG) Z5031-a national trial of chemoradiation following pancreaticoduodenectomy (PD)-were rigorously evaluated. We analyzed variables with the potential to influence staging or outcome.
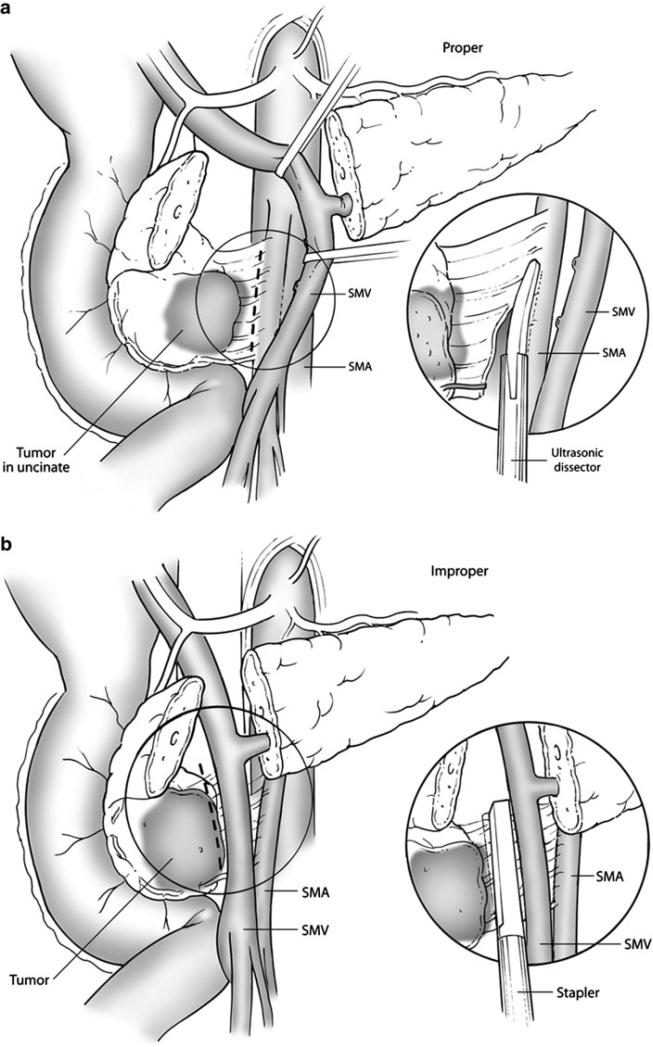
Results: 80 patients reported to have undergone R0 (75%) or R1 (25%) pylorus-preserving (38%) or standard (62%) PD were evaluated. A search for metastases was documented in 96% of cases. The proximity of the tumor to the superior mesenteric vein was reported in 69%; vein resection was required in 9% and lateral venorrhaphy in 14%. The method of dissection along the superior mesenteric artery (SMA) was described in 68%, being ultrasonic dissection (17%), stapler (24%), and clamp and cut (59%). SMA skeletonization was described in 25%, and absence of disease following resection was documented in 24%. The surgeon reported marking the critical SMA margin in 25%; inking was documented in 65% of cases and evaluation of the SMA margin was reported in 47%. A range of 1-49 lymph nodes was evaluated. Only 34% of pathology reports met College of American Pathologists criteria.
Conclusions: Trials of adjuvant therapy following PD suffer from a lack of standardization and quality control prior to patient enrollment. These data suggest areas for improvement in the design of multidisciplinary treatment protocols.
Figures
References
-
- Howard TJ, Krug JE, Yu J, Zyromski NJ, Schmidt CM, Jacobson LE, et al. A margin-negative R0 resection accomplished with minimal postoperative complications is the surgeon's contribution to long-term survival in pancreatic cancer. J Gastrointest Surg. 2006;10:1338–45. discussion 1345–6. - PubMed
-
- [16 August 2010];Pancreatic adenocarcinoma V.2.2010. NCCN Clinical Practice Guidelines in Oncology. 2009 Available at: http://www.nccn.org/professionals/physicians_gls/PDF/pancreatic.pdf.
-
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg. 1985;120:899–903. - PubMed
-
- Neoptolemos JP, Dunn JA, Stocken DD, Almond J, Link K, Beger H, et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. Lancet. 2001;358:1576–85. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
