

Predictors of bacterial pneumonia in Evaluation of Subcutaneous Interleukin-2 in a Randomized International Trial (ESPRIT)
- PMID: 20812949
- PMCID: PMC3048911
- DOI: 10.1111/j.1468-1293.2010.00875.x
Predictors of bacterial pneumonia in Evaluation of Subcutaneous Interleukin-2 in a Randomized International Trial (ESPRIT)
Abstract
Background and objectives: Bacterial pneumonia still contributes to morbidity/mortality in HIV infection despite effective combination antiretroviral therapy (cART). Evaluation of Subcutaneous Interleukin-2 in a Randomized International Trial (ESPRIT), a trial of intermittent recombinant interleukin-2 (rIL-2) with cART vs. cART alone (control arm) in HIV-infected adults with CD4 counts ≥300cells/μL, offered the opportunity to explore associations between bacterial pneumonia and rIL-2, a cytokine that increases the risk of some bacterial infections.
Methods: Baseline and time-updated factors associated with first-episode pneumonia on study were analysed using multivariate proportional hazards regression models. Information on smoking/pneumococcal vaccination history was not collected.
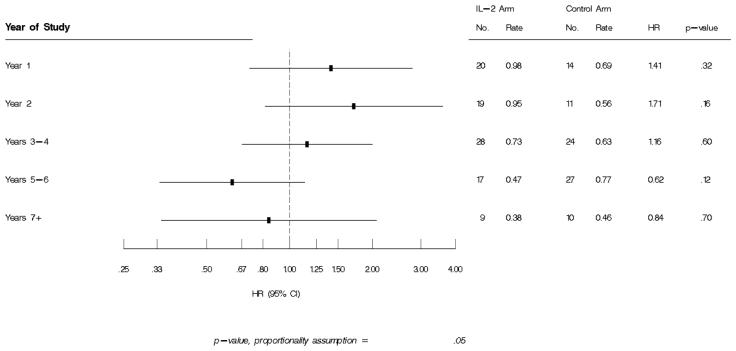
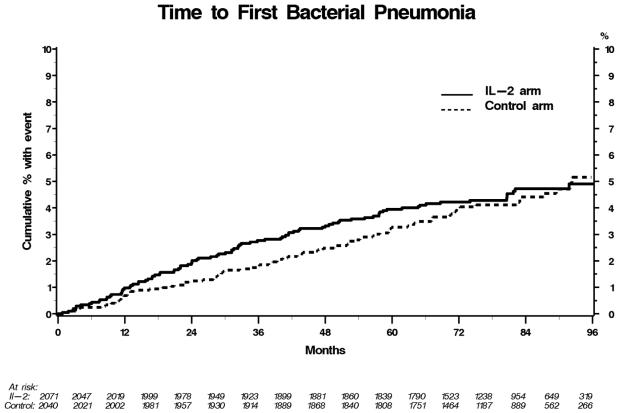
Results: IL-2 cycling was most intense in years 1-2. Over ≈7 years, 93 IL-2 [rate 0.67/100 person-years (PY)] and 86 control (rate 0.63/100 PY) patients experienced a pneumonia event [hazard ratio (HR) 1.06; 95% confidence interval (CI) 0.79, 1.42; P=0.68]. Median CD4 counts prior to pneumonia were 570cells/μL (IL-2 arm) and 463cells/μL (control arm). Baseline risks for bacterial pneumonia included older age, injecting drug use, detectable HIV viral load (VL) and previous recurrent pneumonia; Asian ethnicity was associated with decreased risk. Higher proximal VL (HR for 1 log(10) higher VL 1.28; 95% CI 1.11, 1.47; P<0.001) was associated with increased risk; higher CD4 count prior to the event (HR per 100 cells/μL higher 0.94; 95% CI 0.89, 1.0; P=0.04) decreased risk. Compared with controls, the hazard for a pneumonia event was higher if rIL-2 was received <180 days previously (HR 1.66; 95% CI 1.07, 2.60; P=0.02) vs.≥180 days previously (HR 0.98; 95% CI 0.70, 1.37; P=0.9). Compared with the control group, pneumonia risk in the IL-2 arm decreased over time, with HRs of 1.41, 1.71, 1.16, 0.62 and 0.84 in years 1, 2, 3-4, 5-6 and 7, respectively.
Conclusions: Bacterial pneumonia rates in cART-treated adults with moderate immunodeficiency are high. The mechanism of the association between bacterial pneumonia and recent IL-2 receipt and/or detectable HIV viraemia warrants further exploration.
Trial registration: ClinicalTrials.gov NCT00004978.
© 2010 British HIV Association.
Figures
References
-
- Feikin DR, Feldman C, Schuchat A, Janoff EN. Global strategies to prevent bacterial pneumonia in adults with HIV disease. Lancet Infect Dis. 2004;4(7):445–55. - PubMed
-
- Wallace JM, Rao AV, Glassroth J, Hansen NI, Rosen MJ, Arakaki C, Kvale PA, Reichman LB, Hopewell PC. Respiratory illness in persons with human immunodeficiency virus infection. The Pulmonary Complications of HIV Infection Study Group. Am Rev Respir Dis. 1993;148(6 Pt 1):1523–9. - PubMed
-
- Sullivan JH, Moore RD, Keruly JC, Chaisson RE. Effect of antiretroviral therapy on the incidence of bacterial pneumonia in patients with advanced HIV infection. Am J Respir Crit Care Med. 2000;162(1):64–7. - PubMed
-
- Nagappan V, Kazanjian P. Bacterial infections in adult HIV-infected patients. HIV Clin Trials. 2005;6(4):213–28. Review. - PubMed
-
- Sogaard OS, Lohse N, Gerstoft J, et al. Hospitalization for pneumonia among individuals with and without HIV infection, 1995-2007: a Danish population-based, nationwide cohort study. Clin Infect Dis. 2008;47(10):1345–53. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
