

Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction
- PMID: 20813282
- PMCID: PMC2950645
- DOI: 10.1016/j.jacc.2010.03.077
Global cardiovascular reserve dysfunction in heart failure with preserved ejection fraction
Abstract
Objectives: The purpose of this study was to comprehensively examine cardiovascular reserve function with exercise in patients with heart failure and preserved ejection fraction (HFpEF).
Background: Optimal exercise performance requires an integrated physiologic response, with coordinated increases in heart rate, contractility, lusitropy, arterial vasodilation, endothelial function, and venous return. Cardiac and vascular responses are coupled, and abnormalities in several components may interact to promote exertional intolerance in HFpEF.
Methods: Subjects with HFpEF (n = 21), hypertension without heart failure (n = 19), and no cardiovascular disease (control, n = 10) were studied before and during exercise with characterization of cardiovascular reserve function by Doppler echocardiography, peripheral arterial tonometry, and gas exchange.
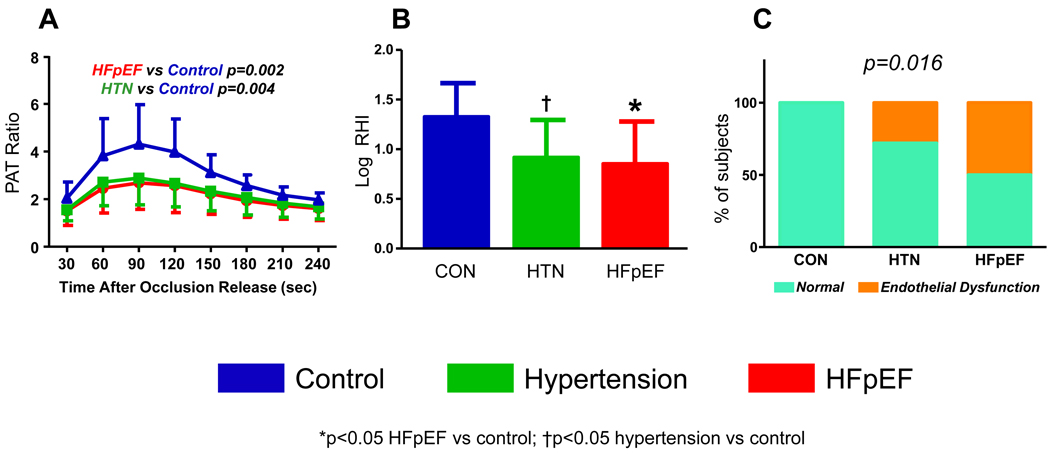
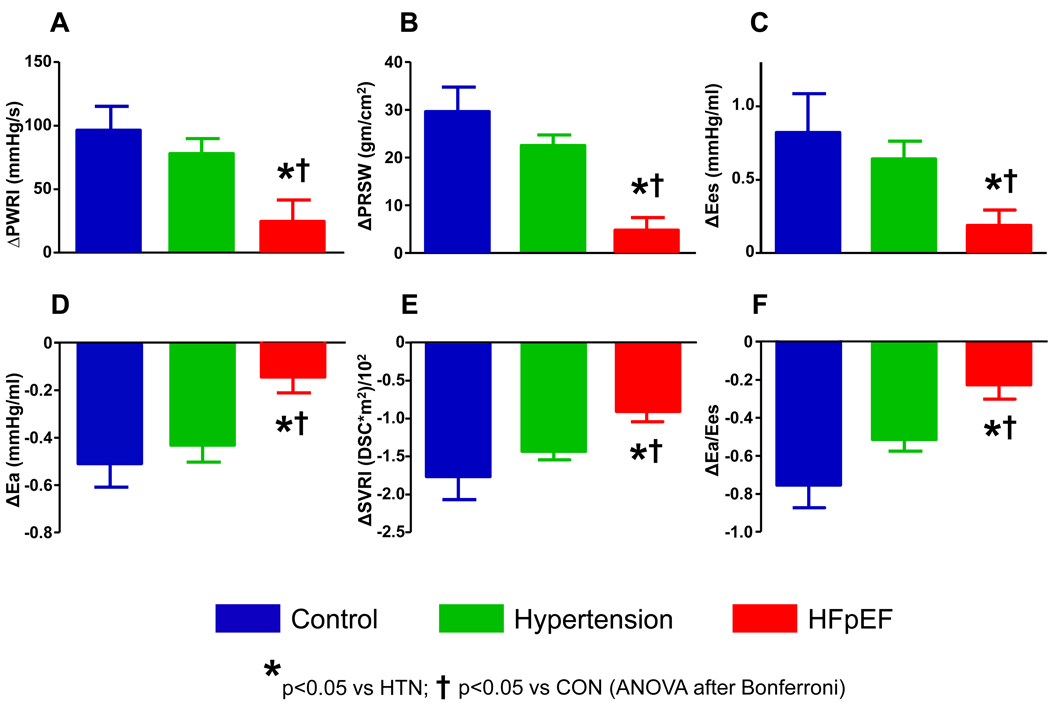
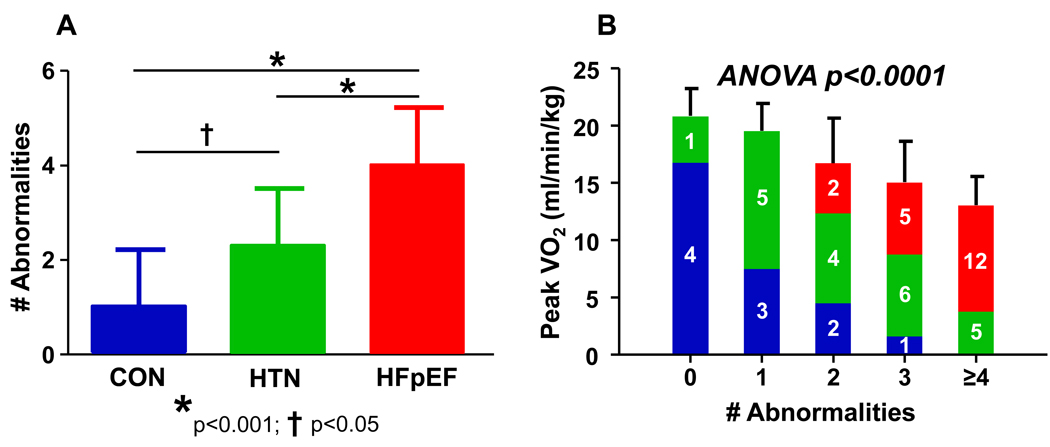
Results: Exercise capacity and tolerance were reduced in HFpEF compared with hypertensive subjects and controls, with lower VO(2) and cardiac index at peak, and more severe dyspnea and fatigue at matched low-level workloads. Endothelial function was impaired in HFpEF and in hypertensive subjects as compared with controls. However, blunted exercise-induced increases in chronotropy, contractility, and vasodilation were unique to HFpEF and resulted in impaired dynamic ventricular-arterial coupling responses during exercise. Exercise capacity and symptoms of exertional intolerance were correlated with abnormalities in each component of cardiovascular reserve function, and HFpEF subjects were more likely to display multiple abnormalities in reserve.
Conclusions: HFpEF is characterized by depressed reserve capacity involving multiple domains of cardiovascular function, which contribute in an integrated fashion to produce exercise limitation. Appreciation of the global nature of reserve dysfunction in HFpEF will better inform optimal design for future diagnostic and therapeutic strategies.
Copyright © 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Culprit Mechanism(s) for Exercise Intolerance in Heart Failure With Normal Ejection Fraction.J Am Coll Cardiol. 2010 Sep 7;56(11):864-6. doi: 10.1016/j.jacc.2010.04.041. J Am Coll Cardiol. 2010. PMID: 20813284 No abstract available.
-
Heart failure with normal ejection fraction: the diagnostic importance of left atrial volume.J Am Coll Cardiol. 2011 Mar 29;57(13):1499; author replies 1499-500. doi: 10.1016/j.jacc.2010.10.046. J Am Coll Cardiol. 2011. PMID: 21435524 No abstract available.
References
-
- Kitzman DW, Little WC, Brubaker PH, et al. Pathophysiological characterization of isolated diastolic heart failure in comparison to systolic heart failure. Jama. 2002;288:2144–2150. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355:251–259. - PubMed
-
- Borlaug BA, Melenovsky V, Russell SD, et al. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation. 2006;114:2138–2147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
