

Neurobehavioral dynamics following chronic sleep restriction: dose-response effects of one night for recovery
- PMID: 20815182
- PMCID: PMC2910531
- DOI: 10.1093/sleep/33.8.1013
Neurobehavioral dynamics following chronic sleep restriction: dose-response effects of one night for recovery
Abstract
Objective: Establish the dose-response relationship between increasing sleep durations in a single night and recovery of neurobehavioral functions following chronic sleep restriction.
Design: Intent-to-treat design in which subjects were randomized to 1 of 6 recovery sleep doses (0, 2, 4, 6, 8, or 10 h TIB) for 1 night following 5 nights of sleep restriction to 4 h TIB.
Setting: Twelve consecutive days in a controlled laboratory environment.
Participants: N = 159 healthy adults (aged 22-45 y), median = 29 y).
Interventions: Following a week of home monitoring with actigraphy and 2 baseline nights of 10 h TIB, subjects were randomized to either sleep restriction to 4 h TIB per night for 5 nights followed by randomization to 1 of 6 nocturnal acute recovery sleep conditions (N = 142), or to a control condition involving 10 h TIB on all nights (N = 17).
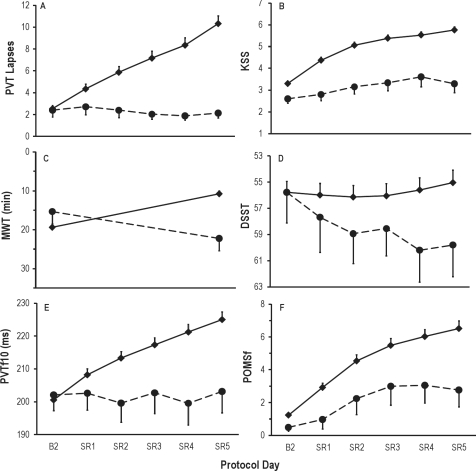
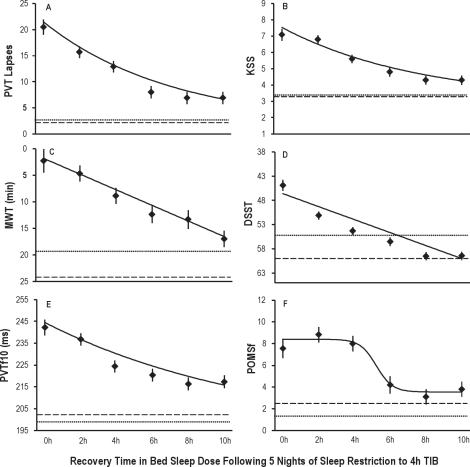
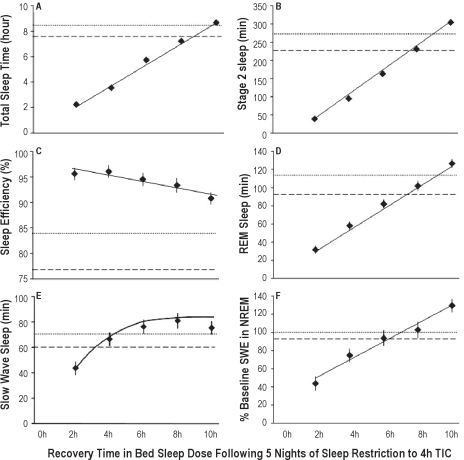
Measurements and results: Primary neurobehavioral outcomes included lapses on the Psychomotor Vigilance Test (PVT), subjective sleepiness from the Karolinska Sleepiness Scale (KSS), and physiological sleepiness from a modified Maintenance of Wakefulness Test (MWT). Secondary outcomes included psychomotor and cognitive speed as measured by PVT fastest RTs and number correct on the Digit Symbol Substitution Task (DSST), respectively, and subjective fatigue from the Profile of Mood States (POMS). The dynamics of neurobehavioral outcomes following acute recovery sleep were statistically modeled across the 0 h-10 h recovery sleep doses. While TST, stage 2, REM sleep and NREM slow wave energy (SWE) increased linearly across recovery sleep doses, best-fitting neurobehavioral recovery functions were exponential across recovery sleep doses for PVT and KSS outcomes, and linear for the MWT. Analyses based on return to baseline and on estimated intersection with control condition means revealed recovery was incomplete at the 10 h TIB (8.96 h TST) for PVT performance, KSS sleepiness, and POMS fatigue. Both TST and SWE were elevated above baseline at the maximum recovery dose of 10 h TIB.
Conclusions: Neurobehavioral deficits induced by 5 nights of sleep restricted to 4 h improved monotonically as acute recovery sleep dose increased, but some deficits remained after 10 h TIB for recovery. Complete recovery from such sleep restriction may require a longer sleep period during 1 night, and/or multiple nights of recovery sleep. It appears that acute recovery from chronic sleep restriction occurs as a result of elevated sleep pressure evident in both increased SWE and TST.
Figures

References
-
- Dinges DF, Maislin G, Brewster RM, et al. Journal of the Transportation Research Board. Washington, DC: Transportation Research Board of the National Academies; 2005. Pilot test of fatigue management technologies; pp. 175–182. No. 1922.
-
- Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: Daily temporal patterns of human chronotypes. J Biol Rhythms. 2003;18:80–90. - PubMed
-
- Dijk D-J, Hayes B, Czeisler CA. Dynamics of electroencephalographic sleep spindles and slow wave activity in men: effect of sleep deprivation. Brain Res. 1993;626:190–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
