

Combining ketamine with astrocytic inhibitor as a potential analgesic strategy for neuropathic pain ketamine, astrocytic inhibitor and pain
- PMID: 20815929
- PMCID: PMC2942826
- DOI: 10.1186/1744-8069-6-50
Combining ketamine with astrocytic inhibitor as a potential analgesic strategy for neuropathic pain ketamine, astrocytic inhibitor and pain
Abstract
Background: Neuropathic pain is an intractable clinical problem. Intrathecal ketamine, a noncompetitive N-methyl-D-aspartate receptor (NMDAR) antagonist, is reported to be useful for treating neuropathic pain in clinic by inhibiting the activity of spinal neurons. Nevertheless, emerging studies have disclosed that spinal astrocytes played a critical role in the initiation and maintenance of neuropathic pain. However, the present clinical therapeutics is still just concerning about neuronal participation. Therefore, the present study is to validate the coadministration effects of a neuronal noncompetitive N-methyl-D-aspartate receptor (NMDAR) antagonist ketamine and astrocytic cytotoxin L-α-aminoadipate (LAA) on spinal nerve ligation (SNL)-induced neuropathic pain.
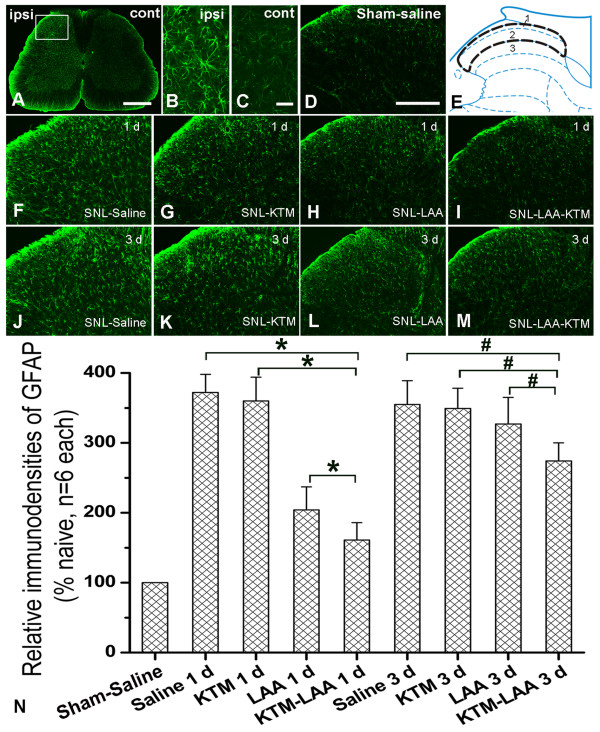
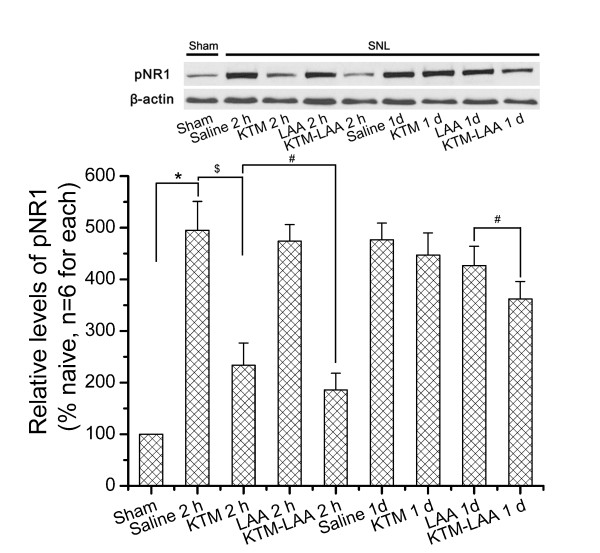
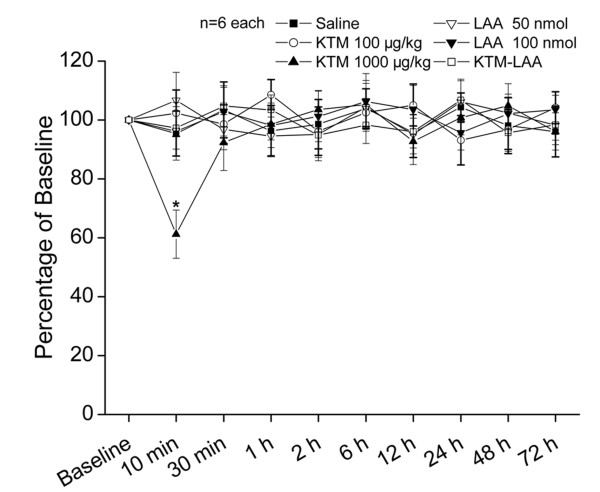
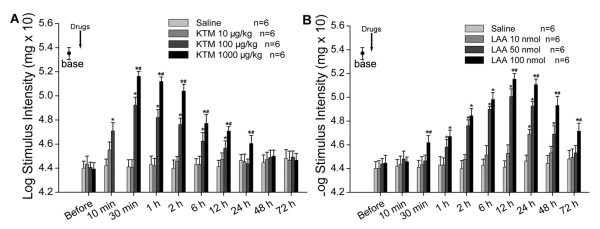
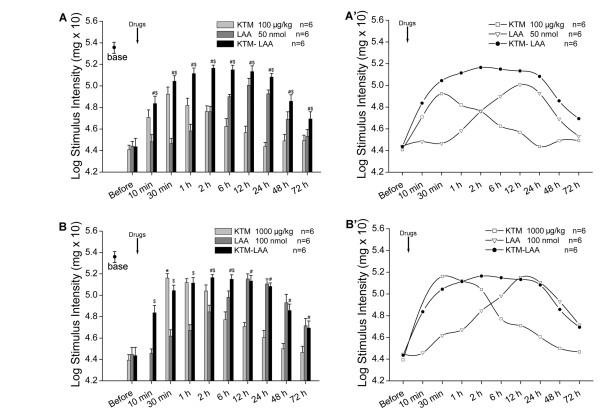
Results: Intrathecal ketamine (10, 100, 1000 μg/kg) or LAA (10, 50, 100 nmol) alleviated SNL-induced mechanical allodynia in a dose-dependent manner respectively. Phosphorylated NR1 (pNR1) or glial fibrillary acidic protein (GFAP) expression was down-regulated by intrathecal ketamine (100, 1000 μg/kg) or LAA (50, 100 nmol) respectively. The combination of ketamine (100 μg/kg) with LAA (50 nmol) showed superadditive effects on neuropathic pain compared with that of intrathecal administration of either ketamine or LAA alone. Combined administration obviously relieved mechanical allodynia in a quick and stable manner. Moreover, down-regulation of pNR1 and GFAP expression were also enhanced by drugs coadministration.
Conclusions: These results suggest that combining NMDAR antagonist ketamine with an astrocytic inhibitor or cytotoxin, which is suitable for clinical use once synthesized, might be a potential strategy for clinical management of neuropathic pain.
Figures
References
-
- Xing GG, Liu FY, Qu XX, Han JS, Wan Y. Long-term synaptic plasticity in the spinal dorsal horn and its modulation by electroacupuncture in rats with neuropathic pain. Exp Neurol. 2007;208:323–332. - PubMed
-
- Kiefer RT, Rohr P, Ploppa A, Dieterich HJ, Grothusen J, Koffler S, Altemeyer KH, Unertl K, Schwartzman RJ. Efficacy of Ketamine in Anesthetic Dosage for the Treatment of Refractory Complex Regional Pain Syndrome: An Open-Label Phase II Study. Pain Med. 2008;9:1173–1201. doi: 10.1111/j.1526-4637.2007.00402.x. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
