

Three-dimensional surgical simulation
- PMID: 20816308
- PMCID: PMC2994415
- DOI: 10.1016/j.ajodo.2009.08.026
Three-dimensional surgical simulation
Abstract
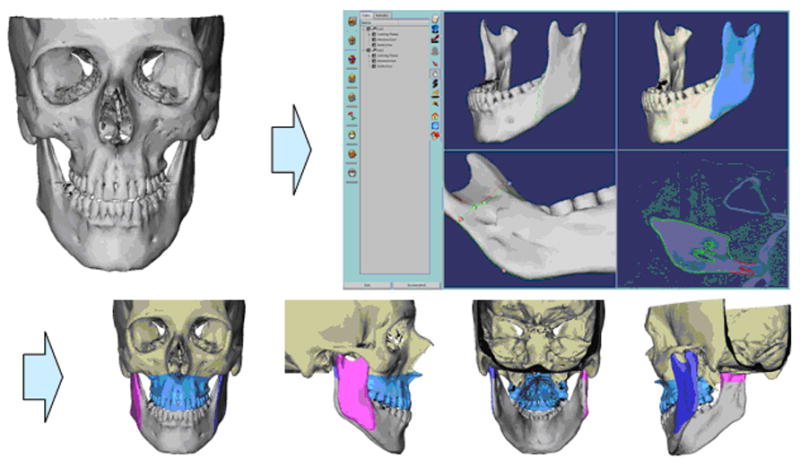
In this article, we discuss the development of methods for computer-aided jaw surgery, which allows us to incorporate the high level of precision necessary for transferring virtual plans into the operating room. We also present a complete computer-aided surgery system developed in close collaboration with surgeons. Surgery planning and simulation include construction of 3-dimensional surface models from cone-beam computed tomography, dynamic cephalometry, semiautomatic mirroring, interactive cutting of bone, and bony segment repositioning. A virtual setup can be used to manufacture positioning splints for intraoperative guidance. The system provides further intraoperative assistance with a computer display showing jaw positions and 3-dimensional positioning guides updated in real time during the surgical procedure. The computer-aided surgery system aids in dealing with complex cases with benefits for the patient, with surgical practice, and for orthodontic finishing. Advanced software tools for diagnosis and treatment planning allow preparation of detailed operative plans, osteotomy repositioning, bone reconstructions, surgical resident training, and assessing the difficulties of the surgical procedures before the surgery. Computer-aided surgery can make the elaboration of the surgical plan a more flexible process, increase the level of detail and accuracy of the plan, yield higher operative precision and control, and enhance documentation of cases.
2010 American Association of Orthodontists. Published by Mosby, Inc. All rights reserved.
Conflict of interest statement
There is no conflict of interest for any of the contributing authors.
Figures






References
-
- Caloss R, Atkins K, Stella JP. Three-dimensional imaging for virtual assessment and treatment simulation in orthognathic surgery. Oral Maxillofac Surg Clin North Am. 2007;19(3):287–309. v. - PubMed
-
- Altobelli DE, Kikinis R, Mulliken JB, Cline H, Lorensen W, Jolesz F. Computer-assisted three-dimensional planning in craniofacial surgery. Plast Reconstr Surg. 1993;92(4):576–85. discussion 586–7. - PubMed
-
- Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Development of a compact computed tomographic apparatus for dental use. Dentomaxillofac Radiol. 1999;28(4):245–8. - PubMed
-
- Chapuis J. Computer-Aided Cranio-Maxillofacial Surgery. University of Bern; 2006. PhD thesis.
-
- Chapuis J, Schramm A, Pappas I, Hallermann W, Schwenzer-Zimmerer K, Langlotz F, et al. A new system for computer-aided preoperative planning and intraoperative navigation during corrective jaw surgery. IEEE Trans Inf Technol Biomed. 2007;11(3):274–87. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
