

Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomised controlled trial
- PMID: 20817247
- PMCID: PMC2958259
- DOI: 10.1016/S0140-6736(10)61303-7
Oral sucrose as an analgesic drug for procedural pain in newborn infants: a randomised controlled trial
Abstract
Background: Many infants admitted to hospital undergo repeated invasive procedures. Oral sucrose is frequently given to relieve procedural pain in neonates on the basis of its effect on behavioural and physiological pain scores. We assessed whether sucrose administration reduces pain-specific brain and spinal cord activity after an acute noxious procedure in newborn infants.
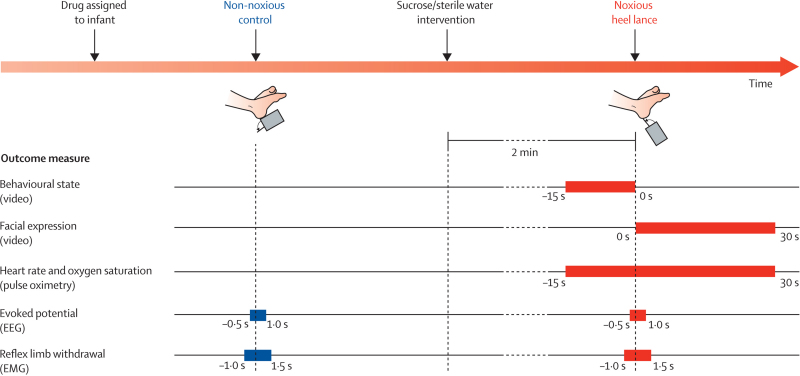
Methods: In this double-blind, randomised controlled trial, 59 newborn infants at University College Hospital (London, UK) were randomly assigned to receive 0·5 mL 24% sucrose solution or 0·5 mL sterile water 2 min before undergoing a clinically required heel lance. Randomisation was by a computer-generated randomisation code, and researchers, clinicians, participants, and parents were masked to the identity of the solutions. The primary outcome was pain-specific brain activity evoked by one time-locked heel lance, recorded with electroencephalography and identified by principal component analysis. Secondary measures were baseline behavioural and physiological measures, observational pain scores (PIPP), and spinal nociceptive reflex withdrawal activity. Data were analysed per protocol. This study is registered, number ISRCTN78390996.
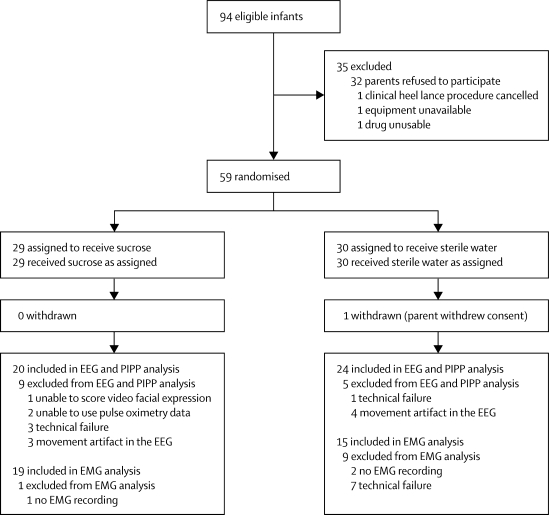
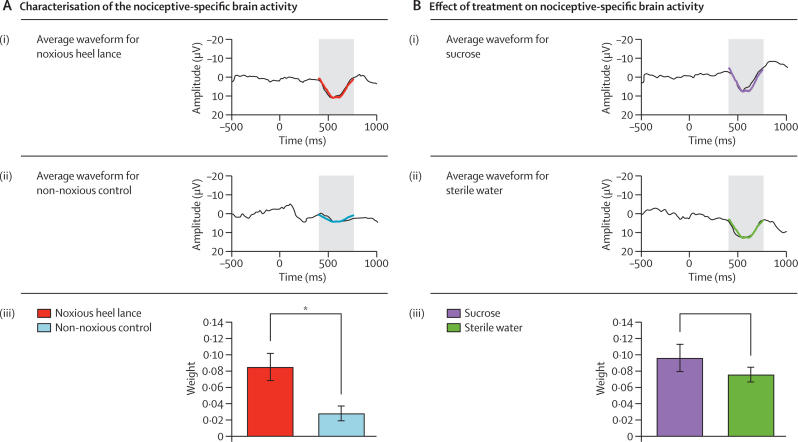
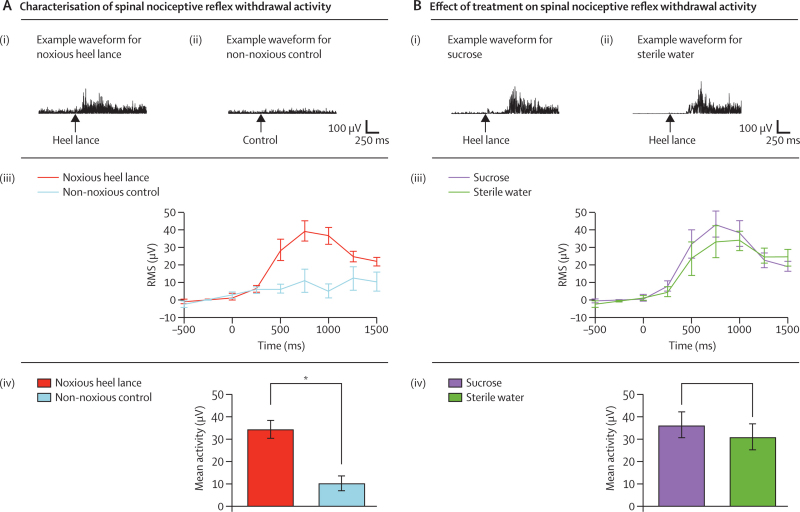
Findings: 29 infants were assigned to receive sucrose and 30 to sterilised water; 20 and 24 infants, respectively, were included in the analysis of the primary outcome measure. Nociceptive brain activity after the noxious heel lance did not differ significantly between infants who received sucrose and those who received sterile water (sucrose: mean 0·10, 95% CI 0·04-0·16; sterile water: mean 0·08, 0·04-0·12; p=0·46). No significant difference was recorded between the sucrose and sterile water groups in the magnitude or latency of the spinal nociceptive reflex withdrawal recorded from the biceps femoris of the stimulated leg. The PIPP score was significantly lower in infants given sucrose than in those given sterile water (mean 5·8, 95% CI 3·7-7·8 vs 8·5, 7·3-9·8; p=0·02) and significantly more infants had no change in facial expression after sucrose administration (seven of 20 [35%] vs none of 24; p<0·0001).
Interpretation: Our data suggest that oral sucrose does not significantly affect activity in neonatal brain or spinal cord nociceptive circuits, and therefore might not be an effective analgesic drug. The ability of sucrose to reduce clinical observational scores after noxious events in newborn infants should not be interpreted as pain relief.
Funding: Medical Research Council.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Is sucrose an effective analgesic for newborn babies?Lancet. 2010 Oct 9;376(9748):1201-3. doi: 10.1016/S0140-6736(10)61358-X. Lancet. 2010. PMID: 20817245 No abstract available.
-
Oral sucrose for procedural pain in infants.Lancet. 2011 Jan 1;377(9759):25; author reply 27-8. doi: 10.1016/S0140-6736(10)62330-6. Lancet. 2011. PMID: 21195240 No abstract available.
-
Oral sucrose for procedural pain in infants.Lancet. 2011 Jan 1;377(9759):25; author reply 27-8. doi: 10.1016/S0140-6736(10)62329-X. Lancet. 2011. PMID: 21195241 No abstract available.
-
Oral sucrose for procedural pain in infants.Lancet. 2011 Jan 1;377(9759):25-6; author reply 27-8. doi: 10.1016/S0140-6736(10)62331-8. Lancet. 2011. PMID: 21195242 No abstract available.
-
Oral sucrose for procedural pain in infants.Lancet. 2011 Jan 1;377(9759):26-7; author reply 27-8. doi: 10.1016/S0140-6736(10)62333-1. Lancet. 2011. PMID: 21195243 No abstract available.
-
Oral sucrose for procedural pain in infants.Lancet. 2011 Jan 1;377(9759):26; author reply 27-8. doi: 10.1016/S0140-6736(10)62332-X. Lancet. 2011. PMID: 21195244 No abstract available.
References
-
- Anand KJ. Consensus statement for the prevention and management of pain in the newborn. Arch Pediatr Adolesc Med. 2001;155:173–180. - PubMed
-
- Stevens B, Yamada J, Ohlsson A. Sucrose for analgesia in newborn infants undergoing painful procedures. Cochrane Database Syst Rev. 2010;1 CD001069. - PubMed
-
- Carbajal R, Rousset A, Danan C. Epidemiology and treatment of painful procedures in neonates in intensive care units. JAMA. 2008;300:60–70. - PubMed
-
- Simons SH, van DM, Anand KS, Roofthooft D, van Lingen RA, Tibboel D. Do we still hurt newborn babies? A prospective study of procedural pain and analgesia in neonates. Arch Pediatr Adolesc Med. 2003;157:1058–1064. - PubMed
-
- Fitzgerald M, Walker SM. Infant pain management: a developmental neurobiological approach. Nat Clin Pract Neurol. 2009;5:35–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
