

Safety and proof of principle study of cerebellar vermal theta burst stimulation in refractory schizophrenia
- PMID: 20817483
- PMCID: PMC3268232
- DOI: 10.1016/j.schres.2010.08.015
Safety and proof of principle study of cerebellar vermal theta burst stimulation in refractory schizophrenia
Abstract
Background: Early invasive electrical stimulation studies suggested that enhancement of cerebellar vermal activity might prove valuable in symptomatic treatment of refractory neuropsychiatric diseases via modulation of emotion and affect. This proof of principle study aimed to test this hypothesis using noninvasive brain stimulation, and to explore the safety of this protocol in schizophrenia.
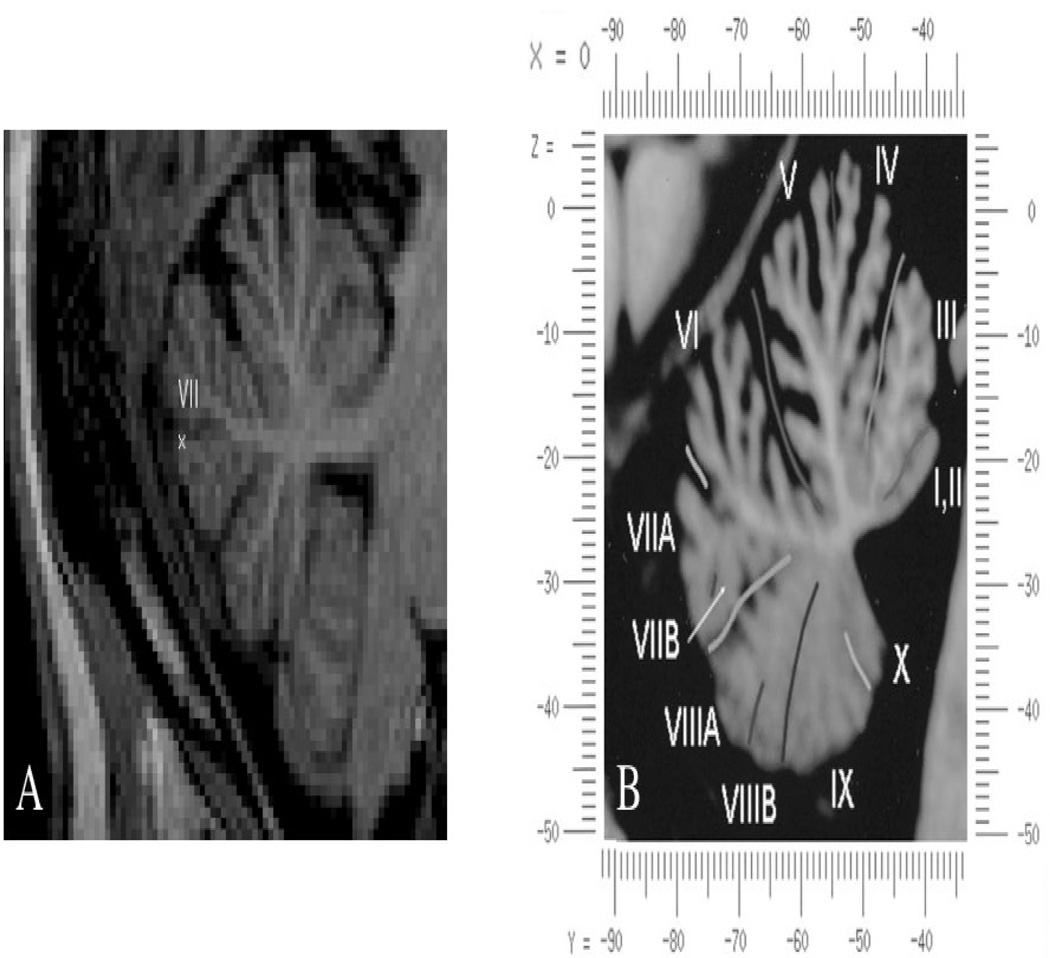
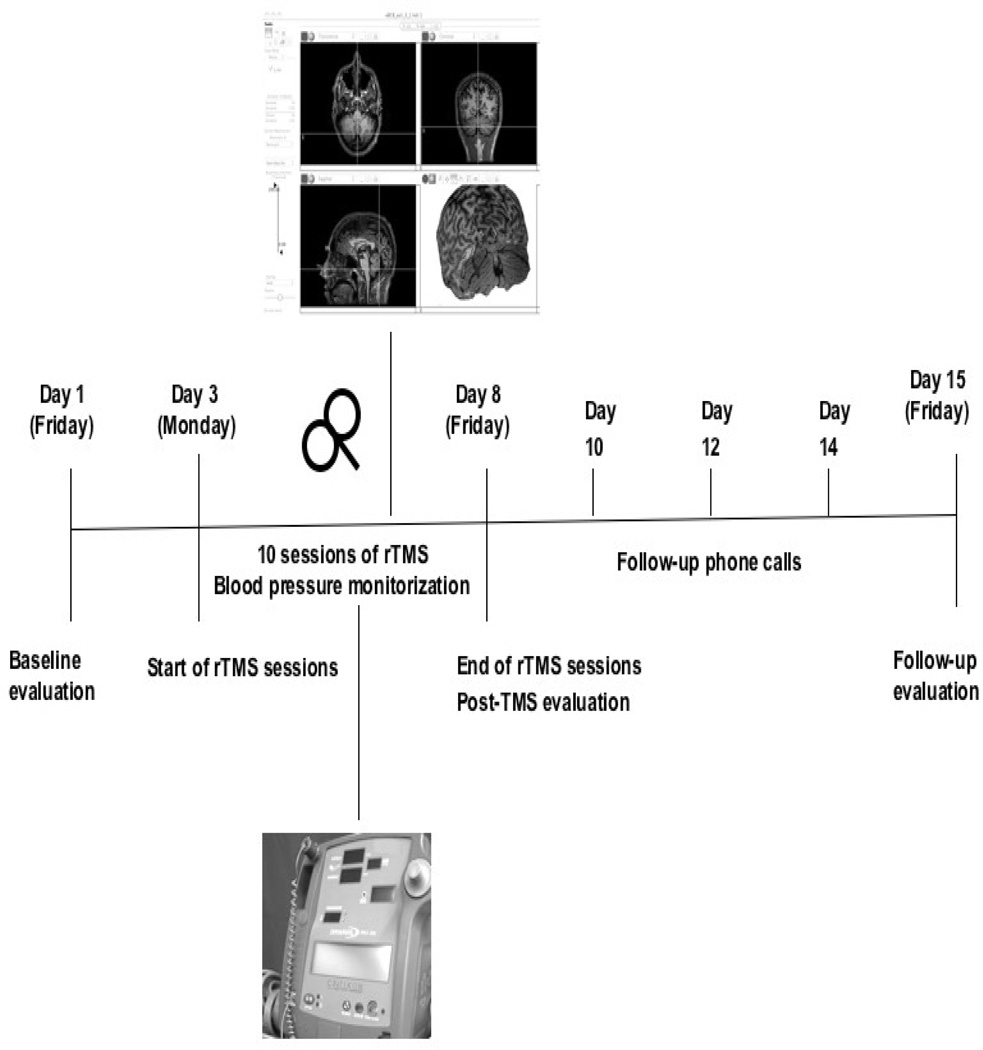
Methods: Eight treatment-refractory patients with schizophrenia underwent ten sessions of intermittent theta burst stimulation (TBS) to the cerebellar vermis using MRI-guided transcranial magnetic stimulation (TMS). Assessments included side effect questionnaires, cardiovascular monitoring, psychiatric evaluations and comprehensive neuropsychological testing before and after TBS and at one-week follow-up.
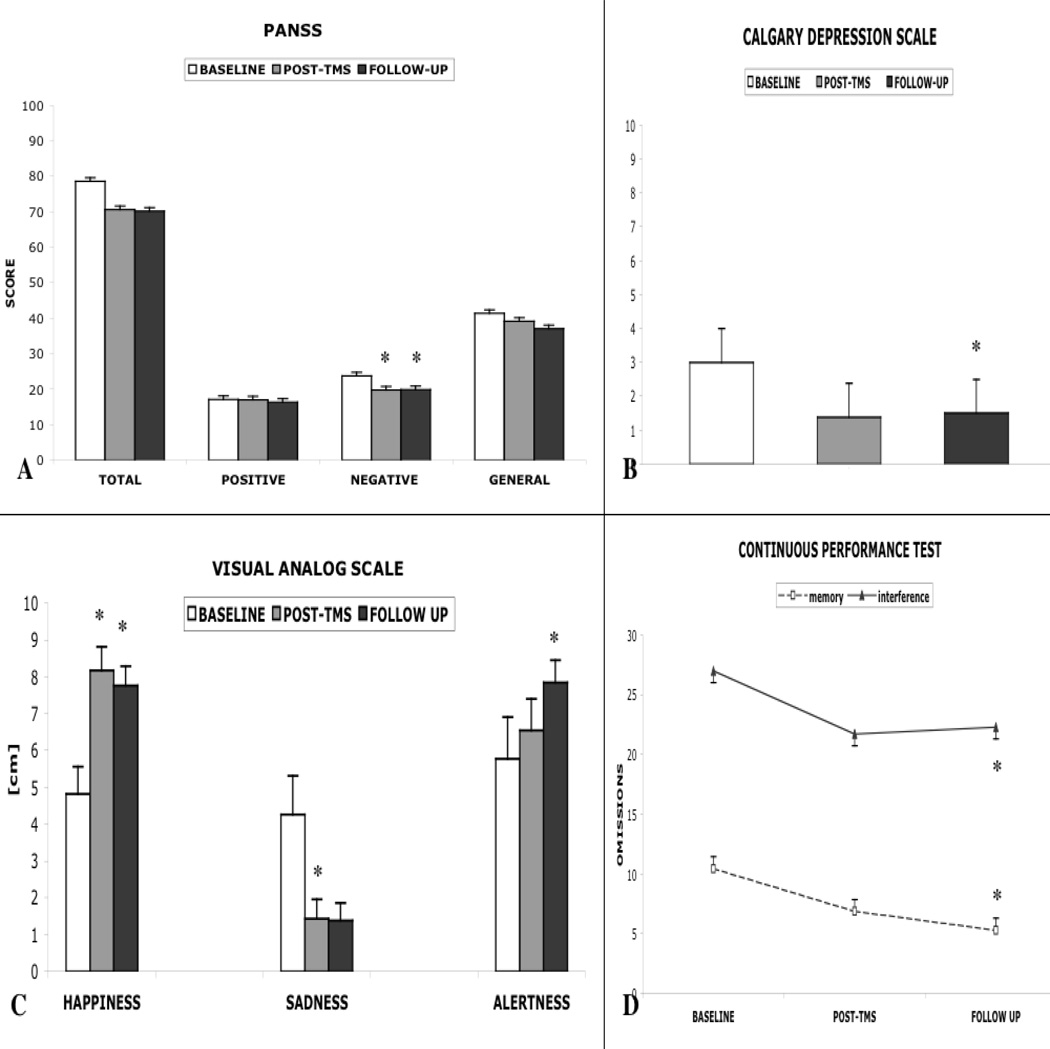
Results: Overall, TBS was tolerated well with mild side effects primarily comprising neck pain and headache. No serious adverse events occurred. Diastolic blood pressure (BP) showed mild decreases for five minutes post-TBS; no significant changes were detected for systolic BP or pulse. PANSS negative subscale showed significant improvements following TBS and during the follow-up. Calgary Depression Scale and self-report visual analog scales for Happiness and Sadness pointed to significant mood elevation. Neuropsychological testing revealed significantly fewer omissions in working memory and interference conditions of a Continuous Performance Test, a longer spatial span and better delay organization on the Rey-Osterrieth Complex Figure during follow-up. No significant worsening in psychiatric or neuropsychological measures was detected.
Conclusions: Theta burst stimulation of the cerebellar vermis is safe and well-tolerated, while offering the potential to modulate affect, emotion and cognition in schizophrenia. Future randomized, sham-stimulation controlled studies are warranted to support the clinical efficacy of this technique.
Copyright © 2010 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Efficacy of Intensive Cerebellar Intermittent Theta Burst Stimulation (iCiTBS) in Treatment-Resistant Schizophrenia: a Randomized Placebo-Controlled Study.Cerebellum. 2021 Feb;20(1):116-123. doi: 10.1007/s12311-020-01193-9. Epub 2020 Sep 22. Cerebellum. 2021. PMID: 32964381 Free PMC article. Clinical Trial.
-
The efficacy of cerebellar vermal deep high frequency (theta range) repetitive transcranial magnetic stimulation (rTMS) in schizophrenia: A randomized rater blind-sham controlled study.Psychiatry Res. 2016 Sep 30;243:413-20. doi: 10.1016/j.psychres.2016.07.023. Epub 2016 Jul 16. Psychiatry Res. 2016. PMID: 27450744 Clinical Trial.
-
Theta-burst rTMS in schizophrenia to ameliorate negative and cognitive symptoms: study protocol for a double-blind, sham-controlled, randomized clinical trial.Trials. 2024 Apr 17;25(1):269. doi: 10.1186/s13063-024-08106-9. Trials. 2024. PMID: 38632647 Free PMC article.
-
Safety Considerations for Cerebellar Theta Burst Stimulation.Clin Ther. 2020 Jul;42(7):1169-1190.e1. doi: 10.1016/j.clinthera.2020.06.001. Epub 2020 Jul 14. Clin Ther. 2020. PMID: 32674957
-
Safety and Efficacy of Theta-Burst Stimulation in the Treatment of Psychiatric Disorders: A Review of the Literature.J Nerv Ment Dis. 2017 Nov;205(11):823-839. doi: 10.1097/NMD.0000000000000742. J Nerv Ment Dis. 2017. PMID: 29077650 Review.
Cited by
-
Cerebellar stimulation in schizophrenia: A systematic review of the evidence and an overview of the methods.Front Psychiatry. 2022 Dec 22;13:1069488. doi: 10.3389/fpsyt.2022.1069488. eCollection 2022. Front Psychiatry. 2022. PMID: 36620688 Free PMC article.
-
Changes in plasticity across the lifespan: cause of disease and target for intervention.Prog Brain Res. 2013;207:91-120. doi: 10.1016/B978-0-444-63327-9.00016-3. Prog Brain Res. 2013. PMID: 24309252 Free PMC article. Review.
-
Neural correlates of positive and negative symptoms through the illness course: an fMRI study in early psychosis and chronic schizophrenia.Sci Rep. 2019 Oct 8;9(1):14444. doi: 10.1038/s41598-019-51023-0. Sci Rep. 2019. PMID: 31595009 Free PMC article.
-
Cerebellar D1DR-expressing neurons modulate the frontal cortex during timing tasks.Neurobiol Learn Mem. 2020 Apr;170:107067. doi: 10.1016/j.nlm.2019.107067. Epub 2019 Aug 9. Neurobiol Learn Mem. 2020. PMID: 31404656 Free PMC article.
-
Cerebellar Cortex as a Therapeutic Target for Neurostimulation.Cerebellum. 2018 Dec;17(6):777-787. doi: 10.1007/s12311-018-0976-8. Cerebellum. 2018. PMID: 30276522 Review.
References
-
- Anand BK, Malhotra CL, Singh B, Dua S. Cerebellar Projections to the Limbic System. J Neurophysiol. 1959;22:451–458. - PubMed
-
- Andreasen NC, O'Leary DS, Flaum M, et al. Hypofrontality in schizophrenia: distributed dysfunctional circuits in neuroleptic-naive patients. Lancet. 1997;349:1730–1734. - PubMed
-
- Andreasen NC, Paradiso S, O'Leary DS. Cognitive dysmetria as an integrative theory of schizophrenia: a dysfunction in cortical-subcortical-cerebellar circuitry? Schizophr Bull. 1998;24:203–218. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
