

Intensive blood-pressure control in hypertensive chronic kidney disease
- PMID: 20818902
- PMCID: PMC3662974
- DOI: 10.1056/NEJMoa0910975
Intensive blood-pressure control in hypertensive chronic kidney disease
Abstract
Background: In observational studies, the relationship between blood pressure and end-stage renal disease (ESRD) is direct and progressive. The burden of hypertension-related chronic kidney disease and ESRD is especially high among black patients. Yet few trials have tested whether intensive blood-pressure control retards the progression of chronic kidney disease among black patients.
Methods: We randomly assigned 1094 black patients with hypertensive chronic kidney disease to receive either intensive or standard blood-pressure control. After completing the trial phase, patients were invited to enroll in a cohort phase in which the blood-pressure target was less than 130/80 mm Hg. The primary clinical outcome in the cohort phase was the progression of chronic kidney disease, which was defined as a doubling of the serum creatinine level, a diagnosis of ESRD, or death. Follow-up ranged from 8.8 to 12.2 years.
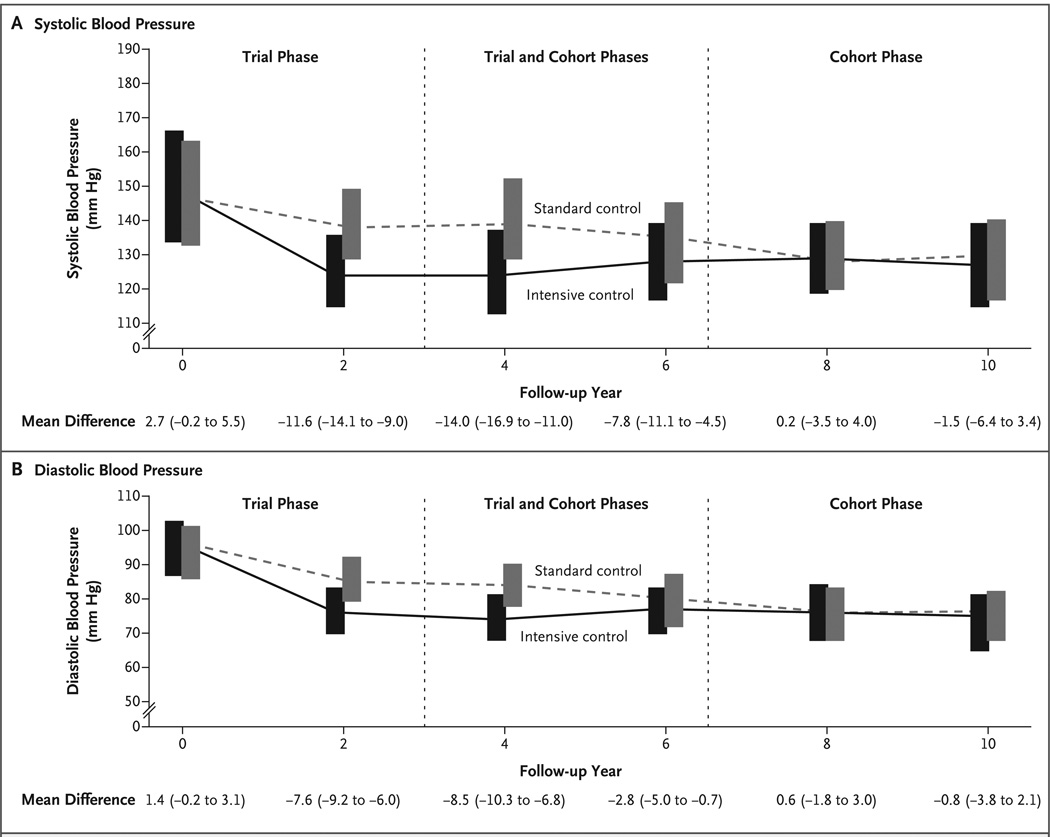
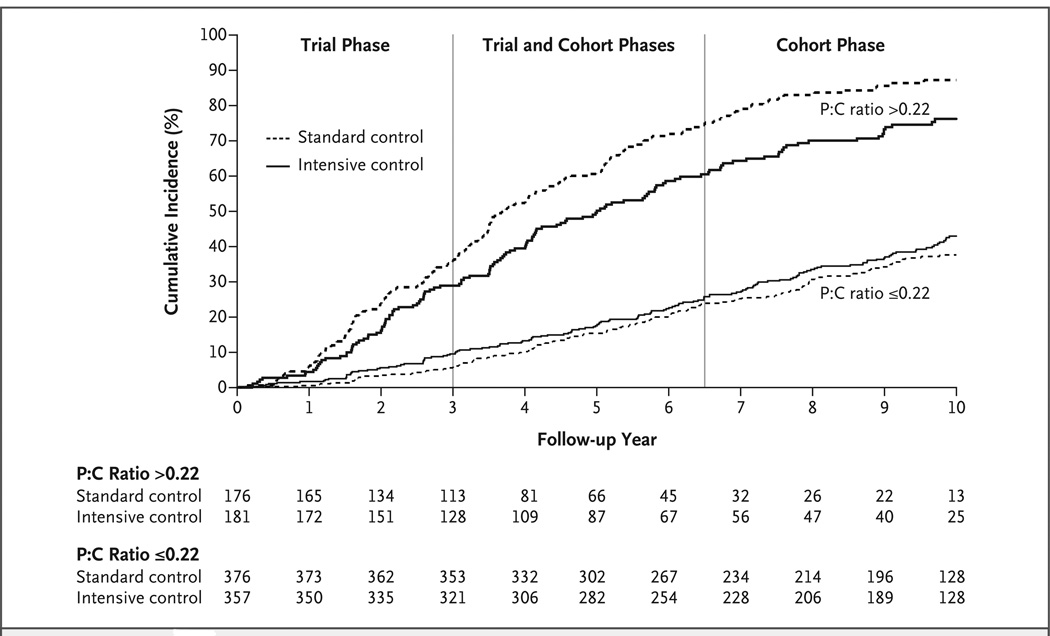
Results: During the trial phase, the mean blood pressure was 130/78 mm Hg in the intensive-control group and 141/86 mm Hg in the standard-control group. During the cohort phase, corresponding mean blood pressures were 131/78 mm Hg and 134/78 mm Hg. In both phases, there was no significant between-group difference in the risk of the primary outcome (hazard ratio in the intensive-control group, 0.91; P=0.27). However, the effects differed according to the baseline level of proteinuria (P=0.02 for interaction), with a potential benefit in patients with a protein-to-creatinine ratio of more than 0.22 (hazard ratio, 0.73; P=0.01).
Conclusions: In overall analyses, intensive blood-pressure control had no effect on kidney disease progression. However, there may be differential effects of intensive blood-pressure control in patients with and those without baseline proteinuria. (Funded by the National Institute of Diabetes and Digestive and Kidney Diseases, the National Center on Minority Health and Health Disparities, and others.)
Figures
Comment in
-
Hypertension control in African-American patients with chronic kidney disease.N Engl J Med. 2010 Sep 2;363(10):974-6. doi: 10.1056/NEJMe1007783. N Engl J Med. 2010. PMID: 20818909 No abstract available.
-
Intensive blood-pressure control in hypertensive chronic kidney disease.N Engl J Med. 2010 Dec 23;363(26):2565; author reply 2565-6. doi: 10.1056/NEJMc1011419. N Engl J Med. 2010. PMID: 21175324 No abstract available.
-
Intensive blood-pressure control in hypertensive chronic kidney disease.N Engl J Med. 2010 Dec 23;363(26):2564-5; author reply 2565-6. doi: 10.1056/NEJMc1011419. N Engl J Med. 2010. PMID: 21175325 No abstract available.
-
Intensive blood-pressure control in hypertensive chronic kidney disease.N Engl J Med. 2010 Dec 23;363(26):2564; author reply 2565-6. doi: 10.1056/NEJMc1011419. N Engl J Med. 2010. PMID: 21175326 No abstract available.
-
How much blood pressure control is beneficial in patients with chronic kidney disease?Curr Hypertens Rep. 2011 Apr;13(2):93-5. doi: 10.1007/s11906-010-0177-4. Curr Hypertens Rep. 2011. PMID: 21210307 No abstract available.
-
African American patients with hypertensive chronic kidney disease receive no benefit on kidney disease progression from the currently recommended blood pressure goal of <130/80 mm Hg unless there is significant proteinuria at baseline: long-term follow-up of the AASK study.J Clin Hypertens (Greenwich). 2011 Mar;13(3):214-6. doi: 10.1111/j.1751-7176.2010.00409.x. Epub 2010 Dec 17. J Clin Hypertens (Greenwich). 2011. PMID: 21366854 Free PMC article. No abstract available.
References
-
- Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038–2047. - PubMed
-
- U.S. Renal Data System. Atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2008.
-
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Stamler J. Endstage renal disease in African-American and white men: 16-year MRFIT findings. JAMA. 1997;277:1293–1298. - PubMed
-
- Klahr S, Levey AS, Beck GJ, et al. The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. N Engl J Med. 1994;330:877–884. - PubMed
-
- Wright JT, Jr, Bakris G, Greene T, et al. Effect of blood pressure lowering and antihy pertensive dr ug class on progression of hypertensive kidney disease: results from the AASK trial. JAMA. 2002;288:2421–2431. [Erratum, JAMA 2006;295:2726.] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- DK 2818-02/DK/NIDDK NIH HHS/United States
- P20-RR11145/RR/NCRR NIH HHS/United States
- M01 RR-00080/RR/NCRR NIH HHS/United States
- RR029887/RR/NCRR NIH HHS/United States
- P20 RR011104/RR/NCRR NIH HHS/United States
- U01 DK048648/DK/NIDDK NIH HHS/United States
- M01 RR008084/RR/NCRR NIH HHS/United States
- P20 RR011145/RR/NCRR NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- U01 DK045386/DK/NIDDK NIH HHS/United States
- 2P20 RR11104/RR/NCRR NIH HHS/United States
- UL1 RR029887/RR/NCRR NIH HHS/United States
- K24 DK002818/DK/NIDDK NIH HHS/United States
- M0100032/PHS HHS/United States
- M01 RR-00071/RR/NCRR NIH HHS/United States
- M01 RR00827/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- M01 RR000080/RR/NCRR NIH HHS/United States
- M01 RR00052/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical