

A large proportion of asymptomatic Plasmodium infections with low and sub-microscopic parasite densities in the low transmission setting of Temotu Province, Solomon Islands: challenges for malaria diagnostics in an elimination setting
- PMID: 20822506
- PMCID: PMC2944341
- DOI: 10.1186/1475-2875-9-254
A large proportion of asymptomatic Plasmodium infections with low and sub-microscopic parasite densities in the low transmission setting of Temotu Province, Solomon Islands: challenges for malaria diagnostics in an elimination setting
Abstract
Background: Many countries are scaling up malaria interventions towards elimination. This transition changes demands on malaria diagnostics from diagnosing ill patients to detecting parasites in all carriers including asymptomatic infections and infections with low parasite densities. Detection methods suitable to local malaria epidemiology must be selected prior to transitioning a malaria control programme to elimination. A baseline malaria survey conducted in Temotu Province, Solomon Islands in late 2008, as the first step in a provincial malaria elimination programme, provided malaria epidemiology data and an opportunity to assess how well different diagnostic methods performed in this setting.
Methods: During the survey, 9,491 blood samples were collected and examined by microscopy for Plasmodium species and density, with a subset also examined by polymerase chain reaction (PCR) and rapid diagnostic tests (RDTs). The performances of these diagnostic methods were compared.
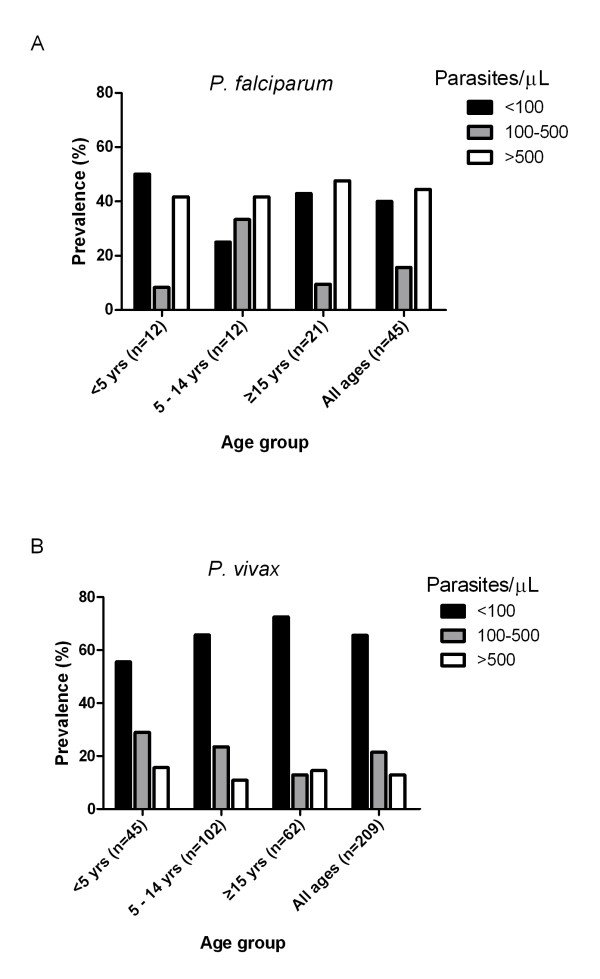
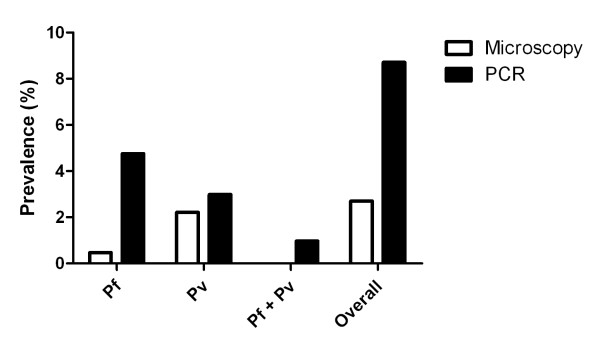
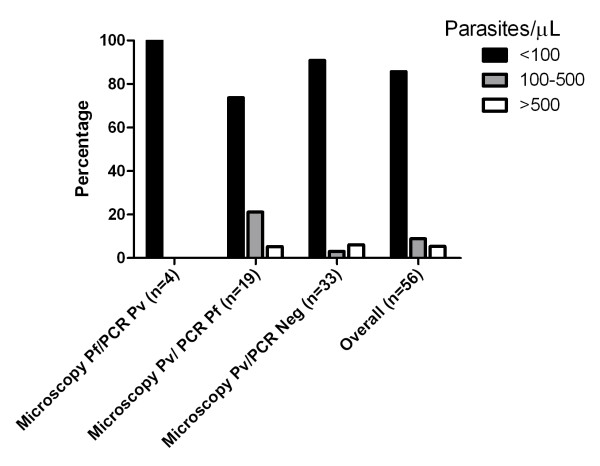
Results: A total of 256 samples were positive by microscopy, giving a point prevalence of 2.7%. The species distribution was 17.5% Plasmodium falciparum and 82.4% Plasmodium vivax. In this low transmission setting, only 17.8% of the P. falciparum and 2.9% of P. vivax infected subjects were febrile (≥ 38°C) at the time of the survey. A significant proportion of infections detected by microscopy, 40% and 65.6% for P. falciparum and P. vivax respectively, had parasite density below 100/μL. There was an age correlation for the proportion of parasite density below 100/μL for P. vivax infections, but not for P. falciparum infections. PCR detected substantially more infections than microscopy (point prevalence of 8.71%), indicating a large number of subjects had sub-microscopic parasitemia. The concordance between PCR and microscopy in detecting single species was greater for P. vivax (135/162) compared to P. falciparum (36/118). The malaria RDT detected the 12 microscopy and PCR positive P. falciparum, but failed to detect 12/13 microscopy and PCR positive P. vivax infections.
Conclusion: Asymptomatic malaria infections and infections with low and sub-microscopic parasite densities are highly prevalent in Temotu province where malaria transmission is low. This presents a challenge for elimination since the large proportion of the parasite reservoir will not be detected by standard active and passive case detection. Therefore effective mass screening and treatment campaigns will most likely need more sensitive assays such as a field deployable molecular based assay.
Figures
References
-
- Wongsrichanalai C, Barcus MJ, Muth S, Sutamihardja A, Wernsdorfer WH. A review of malaria diagnostic tools: microscopy and rapid diagnostic test (RDT) Am J Trop Med Hyg. 2007;77(6 Suppl):119–127. - PubMed
-
- Snounou G, Viriyakosol S, Jarra W, Thaithong S, Brown KN. Identification of the four human malaria parasite species in field samples by the polymerase chain reaction and detection of a high prevalence of mixed infections. Mol Biochem Parasitol. 1993;58:283–292. doi: 10.1016/0166-6851(93)90050-8. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
