

Workshop on idiopathic pulmonary fibrosis in older adults
- PMID: 20822991
- PMCID: PMC4694103
- DOI: 10.1378/chest.09-3006
Workshop on idiopathic pulmonary fibrosis in older adults
Abstract
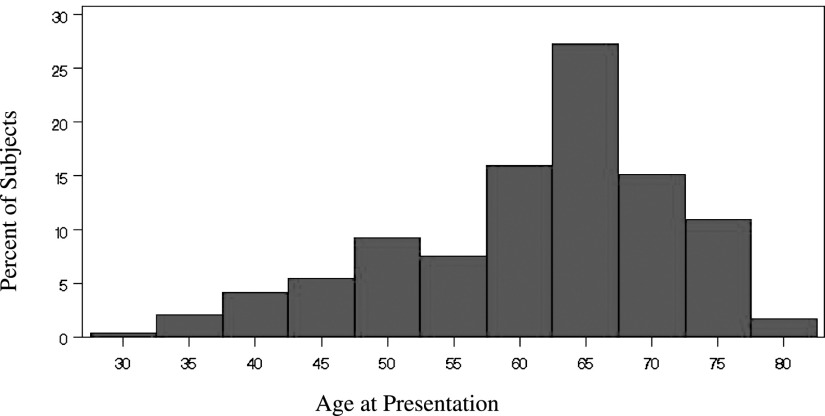
Idiopathic pulmonary fibrosis (IPF), a heterogeneous disease with respect to clinical presentation and rates of progression, disproportionately affects older adults. The diagnosis of IPF is descriptive, based on clinical, radiologic, and histopathologic examination, and definitive diagnosis is hampered by poor interobserver agreement and lack of a consensus definition. There are no effective treatments. Cellular, molecular, genetic, and environmental risk factors have been identified for IPF, but the initiating event and the characteristics of preclinical stages are not known. IPF is predominantly a disease of older adults, and the processes underlying normal aging might significantly influence the development of IPF. Yet, the biology of aging and the principles of medical care for this population have been typically ignored in basic, translational, or clinical IPF research. In August 2009, the Association of Specialty Professors, in collaboration with the American College of Chest Physicians, the American Geriatrics Society, the National Institute on Aging, and the National Heart, Lung, and Blood Institute, held a workshop, summarized herein, to review what is known, to identify research gaps at the interface of aging and IPF, and to suggest priority areas for future research. Efforts to answer the questions identified will require the integration of geriatrics, gerontology, and pulmonary research, but these efforts have great potential to improve care for patients with IPF.
Figures
References
-
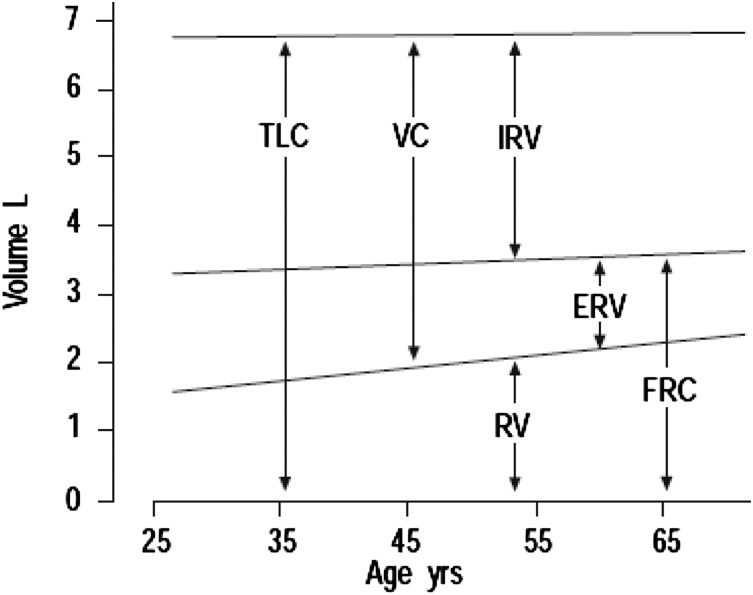
- Griffith KA, Sherrill DL, Siegel EM, Manolio TA, Bonekat HW, Enright PL. Predictors of loss of lung function in the elderly: the Cardiovascular Health Study. Am J Respir Crit Care Med. 2001;163(1):61–68. - PubMed
-
- Brown RH, Pearse DB, Pyrgos G, Liu MC, Togias A, Permutt S. The structural basis of airways hyperresponsiveness in asthma. J Appl Physiol. 2006;101(1):30–39. - PubMed
-
- Harding R, Pinkerton K, Plopper C. The Lung: Development, Aging and the Environment. London, England: Elsevier, Ltd; 2004.
-
- Liebow A. Definition and classification of interstitial pneumonias in human pathology. Prog Respir Res. 1975;8:1–33.
-
- American Thoracic Society European Respiratory Society American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am J Respir Crit Care Med. 2002;165(2):277–304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
