

H-Y antibody titers are increased in unexplained secondary recurrent miscarriage patients and associated with low male : female ratio in subsequent live births
- PMID: 20823116
- PMCID: PMC2955557
- DOI: 10.1093/humrep/deq242
H-Y antibody titers are increased in unexplained secondary recurrent miscarriage patients and associated with low male : female ratio in subsequent live births
Abstract
Background: The birth of a boy is significantly more common than a girl prior to secondary recurrent miscarriage (SRM) and is associated with a poorer chance of a subsequent live birth. Children born after SRM are more likely to be girls. High-titer antisera specific for male antigens (H-Y) have been shown to arrest development of male bovine embryos efficiently. We consequently questioned the role of H-Y antibodies in women with SRM.
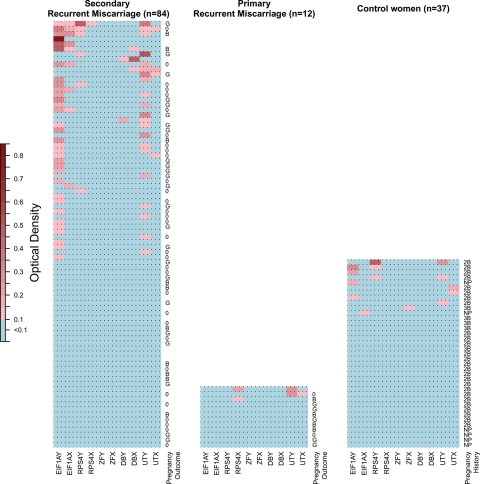
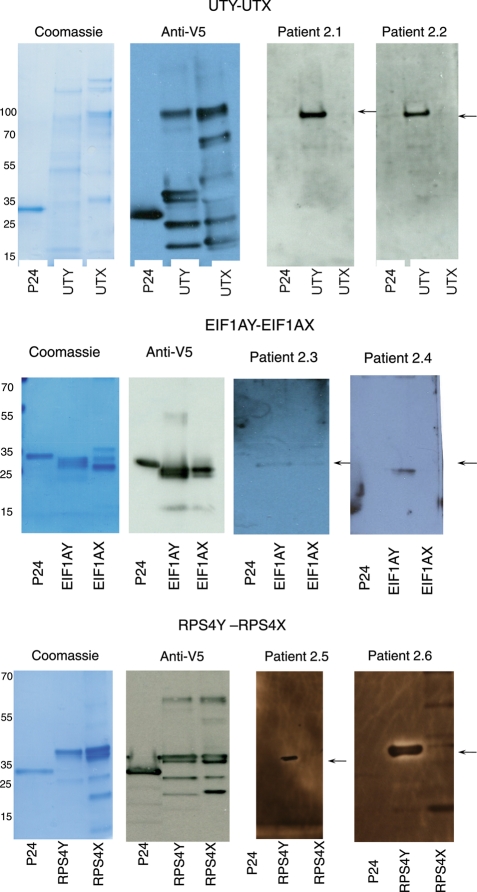
Methods: Serum samples from patients with unexplained SRM (n = 84), unexplained primary recurrent miscarriage (PRM) (n = 12) and healthy women (n = 37) were obtained. The samples were taken during pregnancy (gestational weeks 4-5) for 77 (80%) of the patients. Enzyme-linked immunosorbent assay was used to detect immunoglobulin G antibodies that specifically recognized any of the five recombinant H-Y proteins (EIF1AY, RPS4Y1, ZFY, DDX3Y and UTY) and their H-X homologs.
Results: H-Y-specific antibodies were more frequent in SRM patients (46%) compared with female controls (19%, P = 0.004) and PRM patients (8%, P = 0.01). The presence of H-Y antibodies in early pregnancy was associated with a low male: female birth ratio among the subsequent live births, as only 12% of children born to H-Y antibody-positive patients were boys compared with 44% boys born to H-Y antibody negative patients (P = 0.03).
Conclusions: The high frequency of H-Y antibody-positive SRM patients and the association between the presence of these antibodies in early pregnancy and the low number of male offspring, suggest that maternal immune responses against H-Y antigens can cause pregnancy losses. Further exploring these mechanisms may increase our understanding of unexplained SRM.
Figures
References
-
- Adams KM, Yan Z, Stevens AM, Nelson JL. The changing maternal ‘self’ hypothesis: a mechanism for maternal tolerance of the fetus. Placenta. 2007;28:378–382. doi:10.1016/j.placenta.2006.07.003. - DOI - PubMed
-
- Christiansen OB, Pedersen B, Nielsen HS, Nybo Andersen AM. Impact of the sex of first child on the prognosis in secondary recurrent miscarriage. Hum Reprod. 2004;19:2946–2951. doi:10.1093/humrep/deh516. - DOI - PubMed
-
- Clifton VL. Review: sex and the human placenta: mediating differential strategies of fetal growth and survival. Placenta. 2010;31:S33–S39. - PubMed
-
- Clifton VL, Engel P, Smith R, Gibson P, Brinsmead M, Giles WB. Maternal and neonatal outcomes of pregnancies complicated by asthma in an Australian population. Aust N Z J Obstet Gynaecol. 2009;49:619–626. doi:10.1111/j.1479-828X.2009.01077.x. - DOI - PubMed
-
- Coulam CB, Stephenson M, Stern JJ, Clark DA. Immunotherapy for recurrent pregnancy loss: analysis of results from clinical trials. Am J Reprod Immunol. 1996;35:352–359. - PubMed
