

A multicentre randomised controlled trial of day hospital-based falls prevention programme for a screened population of community-dwelling older people at high risk of falls
- PMID: 20823124
- PMCID: PMC2956530
- DOI: 10.1093/ageing/afq096
A multicentre randomised controlled trial of day hospital-based falls prevention programme for a screened population of community-dwelling older people at high risk of falls
Abstract
Objective: to determine the clinical effectiveness of a day hospital-delivered multifactorial falls prevention programme, for community-dwelling older people at high risk of future falls identified through a screening process.
Design: multicentre randomised controlled trial.
Setting: eight general practices and three day hospitals based in the East Midlands, UK.
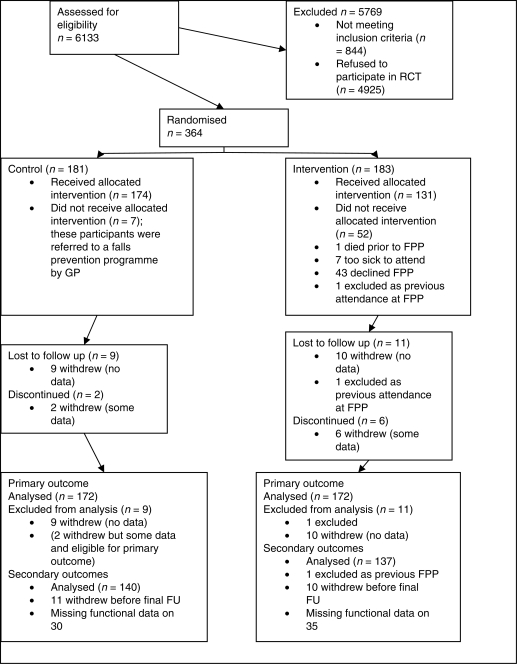
Participants: three hundred and sixty-four participants, mean age 79 years, with a median of three falls risk factors per person at baseline.
Interventions: a day hospital-delivered multifactorial falls prevention programme, consisting of strength and balance training, a medical review and a home hazards assessment.
Main outcome measure: rate of falls over 12 months of follow-up, recorded using self-completed monthly diaries.
Results: one hundred and seventy-two participants in each arm contributed to the primary outcome analysis. The overall falls rate during follow-up was 1.7 falls per person-year in the intervention arm compared with 2.0 falls per person-year in the control arm. The stratum-adjusted incidence rate ratio was 0.86 (95% CI 0.73-1.01), P = 0.08, and 0.73 (95% CI 0.51-1.03), P = 0.07 when adjusted for baseline characteristics. There were no significant differences between the intervention and control arms in any secondary outcomes.
Conclusion: this trial did not conclusively demonstrate the benefit of a day hospital-delivered multifactorial falls prevention programme, in a population of older people identified as being at high risk of a future fall.
Figures
References
-
- Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews. 2009;2 CD007146; doi: 10.1002/14651858.CD007146.pub2. - PubMed
-
- Campbell AJ, Robertson MC. Rethinking individual and community fall prevention strategies: a meta-regression comparing single and multifactorial interventions. Age Ageing. 2007;36:656–62. doi:10.1093/ageing/afm122. - DOI - PubMed
-
- National Institute of Clinical Excellence. Falls: The Assessment and Prevention of Falls in Older People. NICE, London; 2004. - PubMed
-
- Lamb S, Gates S, Fisher J, Cooke M, Carter Y, McCabe C. Scoping Exercise on Fallers’ Clinics: National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO). 2007.
-
- Nandy S, Parsons S, Cryer C, Underwood M. Development and preliminary examination of the predictive validity of the Falls Risk Assessment Tool (FRAT) for use in primary care. J Public Health. 2004;26:138–43. doi:10.1093/pubmed/fdh132. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
