

Cast versus splint in children with minimally angulated fractures of the distal radius: a randomized controlled trial
- PMID: 20823169
- PMCID: PMC2950182
- DOI: 10.1503/cmaj.100119
Cast versus splint in children with minimally angulated fractures of the distal radius: a randomized controlled trial
Abstract
Background: Minimally angulated fractures of the distal radius are common in children and have excellent outcomes. We conducted a randomized controlled trial to determine whether the use of a prefabricated splint is as effective as a cast in the recovery of physical function.
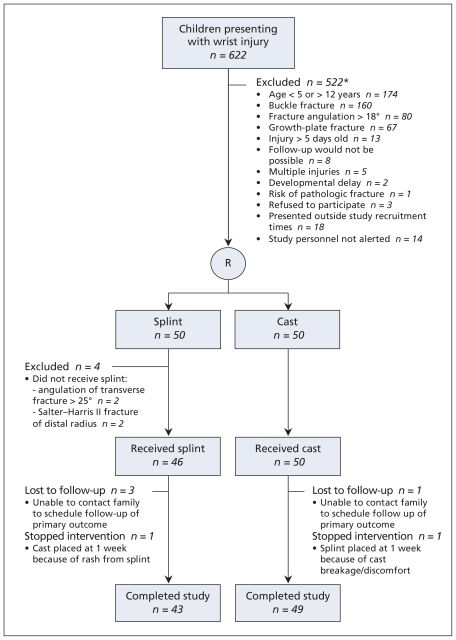
Methods: We included 96 children 5 to 12 years of age who were treated for a minimally angulated (≤ 15°) greenstick or transverse fracture of the wrist between April 2007 and September 2009 at a tertiary care pediatric hospital. Participants were randomly assigned to receive either a prefabricated wrist splint or a short arm cast for four weeks. The primary outcome was physical function at six weeks, measured using the performance version of the Activities Scale for Kids. Additional outcomes included the degree of angulation, range of motion, grip strength and complications.
Results: Of the 96 children, 46 received a splint and 50 a cast. The mean Activities Scale for Kids score at six weeks was 92.8 in the splint group and 91.4 in the cast group (difference 1.44, 95% confidence interval [CI] -1.75 to 4.62). Thus, the null hypothesis that the splint is less effective by at least seven points was rejected. The between-group difference in angulation at four weeks was not statistically significant (9.85° in the splint group and 8.20° in the cast group; mean difference 1.65°, 95% CI -1.82° to 5.11°), nor was the between-group differences in range of motion, grip strength and complications.
Interpretation: In children with minimally angulated fractures of the distal radius, use of a splint was as effective as a cast with respect to the recovery of physical function. In addition, the devices were comparable in terms of the maintenance of fracture stability and the occurrence of complications. (ClinicalTrials.gov trial register no. NCT00610220.).
Figures
Comment in
-
No difference in improvement in physical function between splint and cast at 6 weeks in children with minimally angulated fractures of the distal radius.Evid Based Med. 2011 Apr;16(2):49-50. doi: 10.1136/ebm1161. Epub 2010 Dec 7. Evid Based Med. 2011. PMID: 21139033 No abstract available.
-
Intention-to-treat and per-protocol analysis.CMAJ. 2011 Apr 5;183(6):696; author reply 696. doi: 10.1503/cmaj.111-2033. CMAJ. 2011. PMID: 21464181 Free PMC article. No abstract available.
-
A splint was not inferior to a cast for distal radial fracture in children.J Bone Joint Surg Am. 2011 May 18;93(10):970. doi: 10.2106/JBJS.9310ebo619. J Bone Joint Surg Am. 2011. PMID: 21593375 No abstract available.
References
-
- Bohm ER, Bubbar V, Yong Hing K, et al. Above and below-the-elbow plaster casts for distal forearm fractures in children. A randomized controlled trial. J Bone Joint Surg Am. 2006;88:1–8. - PubMed
-
- Bachman D, Santora S. Orthopedic trauma. In: Fleisher G, Ludwig S, Henretig FM, et al., editors. Textbook of pediatric emergency medicine. Philadelphia (PA): Lippincott Williams & Wilkins; 2000. pp. 1455–7.
-
- Al Ansari K, Howard A, Seeto B, et al. Minimally angulated pediatric wrist fractures: Is casting without manipulation enough? CJEM. 2007;9:9–15. - PubMed
-
- Do TT, Strub WM, Foad SL, et al. Reduction versus remodeling in pediatric distal forearm fractures: a preliminary cost analysis. J Pediatr Orthop B. 2003;12:109–15. - PubMed
-
- Waters PM. Distal radius and ulna fractures. In: Beaty JH, Kasser JR, editors. Fractures in children. Philadelphia (PA): Lippincott Williams & Wilkins; 2001.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous