

Multicenter cluster-randomized trial of a multifactorial intervention to improve antihypertensive medication adherence and blood pressure control among patients at high cardiovascular risk (the COM99 study)
- PMID: 20823391
- PMCID: PMC3001186
- DOI: 10.1161/CIRCULATIONAHA.109.892778
Multicenter cluster-randomized trial of a multifactorial intervention to improve antihypertensive medication adherence and blood pressure control among patients at high cardiovascular risk (the COM99 study)
Abstract
Background: Medication nonadherence is common and results in preventable disease complications. This study assessed the effectiveness of a multifactorial intervention to improve both medication adherence and blood pressure control and to reduce cardiovascular events.
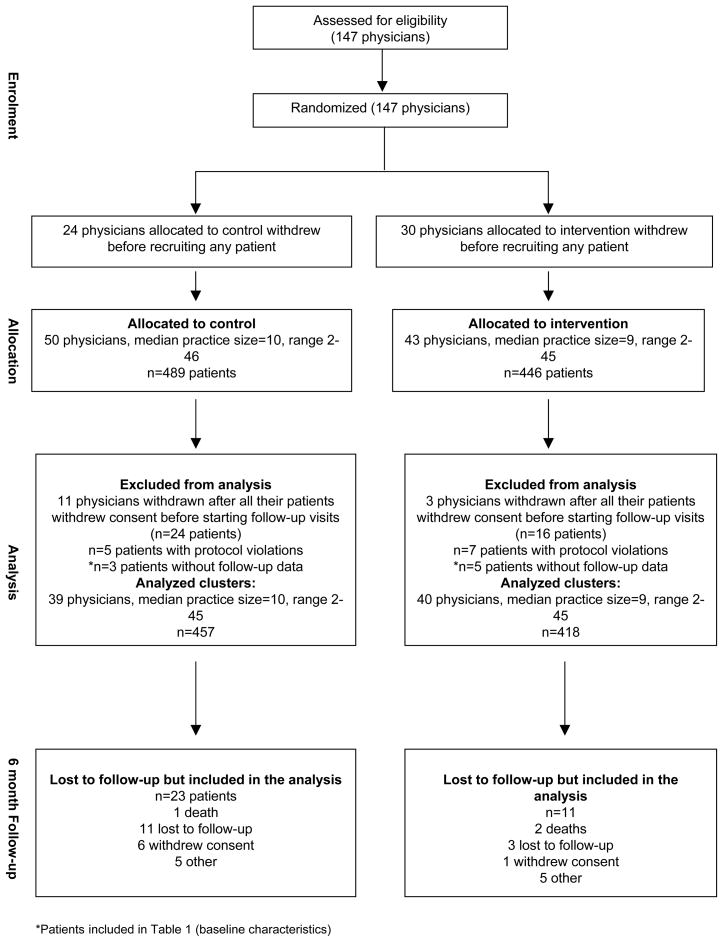
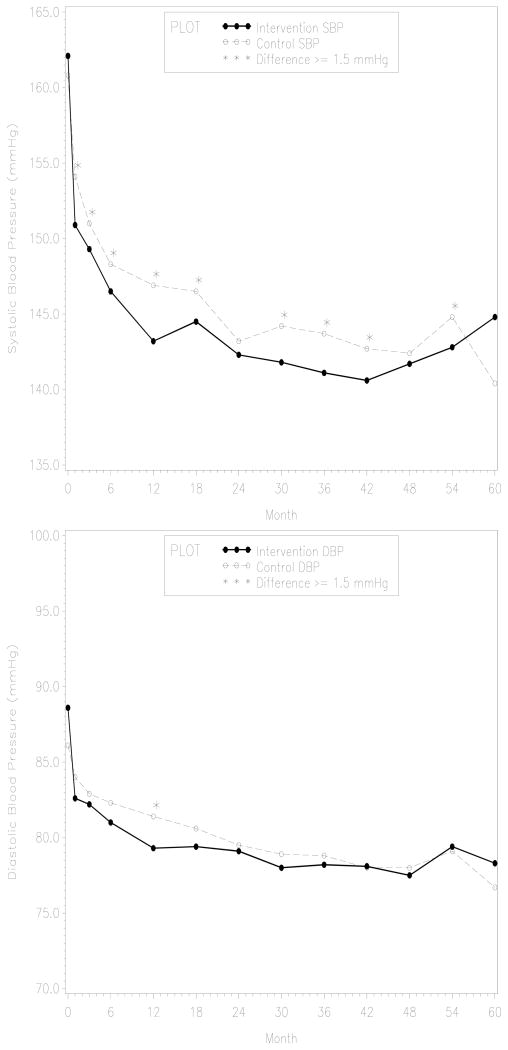
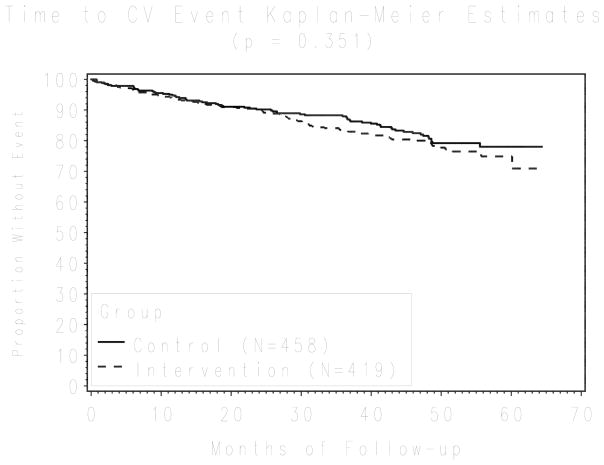
Methods and results: In this multicenter, cluster-randomized trial, physicians from hospital-based hypertension clinics and primary care centers across Spain were randomized to receive and provide the intervention to their high-risk patients. Eligible patients were ≥ 50 years of age, had uncontrolled hypertension, and had an estimated 10-year cardiovascular risk greater than 30%. Physicians randomized to the intervention group counted patients' pills, designated a family member to support adherence behavior, and provided educational information to patients. The primary outcome was blood pressure control at 6 months. Secondary outcomes included both medication adherence and a composite end point of all-cause mortality and cardiovascular-related hospitalizations. Seventy-nine physicians and 877 patients participated in the trial. The mean duration of follow-up was 39 months. Intervention patients were less likely to have an uncontrolled systolic blood pressure (odds ratio 0.62, 95% confidence interval 0.50 to 0.78) and were more likely to be adherent (odds ratio 1.91, 95% confidence interval 1.19 to 3.05) than control group patients at 6 months. After 5 years, 16% of the patients in the intervention group and 19% in the control group met the composite end point (hazard ratio 0.97, 95% confidence interval 0.67 to 1.39).
Conclusions: A multifactorial intervention to improve adherence to antihypertensive medication was effective in improving both adherence and blood pressure control, but it did not appear to improve long-term cardiovascular events.
Conflict of interest statement
Conflicy of Interest Disclosures: None.
Figures
Comment in
-
The search for strategies to control hypertension.Circulation. 2010 Sep 21;122(12):1141-3. doi: 10.1161/CIRCULATIONAHA.110.978759. Epub 2010 Sep 7. Circulation. 2010. PMID: 20823382 Free PMC article. No abstract available.
References
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. - PubMed
-
- Gu Q, Burt VL, Paulose-Ram R, Yoon S, Gillum RF. High Blood Pressure and Cardiovascular Disease Mortality Risk Among U.S. Adults: The Third National Health and Nutrition Examination Survey Mortality Follow-up Study. Annals of Epidemiology. 2008;18:302–309. - PubMed
-
- Wolf-Maier K, Cooper RS, Kramer H, Banegas JR, Giampaoli S, Joffres MR, Poulter N, Primatesta P, Stegmayr B, Thamm M. Hypertension Treatment and Control in Five European Countries, Canada, and the United States. Hypertension. 2004;43:10–17. - PubMed
-
- Jones DW, Hall JE. Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure and Evidence From New Hypertension Trials. Hypertension. 2004;43:1–3. - PubMed
-
- Wong ND, Lopez VA, L’italien G, Chen R, Kline SE, Franklin SS. Inadequate Control of Hypertension in US Adults With Cardiovascular Disease Comorbidities in 2003–2004. Arch Intern Med. 2007;167:2431–2436. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
