

Endoscopy-guided vitreoretinal surgery following penetrating corneal injury: a case report
- PMID: 20823930
- PMCID: PMC2925451
- DOI: 10.2147/opth.s12435
Endoscopy-guided vitreoretinal surgery following penetrating corneal injury: a case report
Abstract
Introduction: Severe ocular trauma requires emergency surgery, and a fresh corneal graft may not always be available. We describe a case of perforating eye injury with corneal opacity, suspected endophthalmitis, and an intraocular foreign body. The patient was successfully treated with a two-step procedure comprising endoscopy-guided vitrectomy followed by corneal transplantation. This surgical technique offers a good option to vitrectomy with simultaneous keratoplasty in emergency cases where no graft is immediately available and there is the possibility of infection due to the presence of a foreign body.
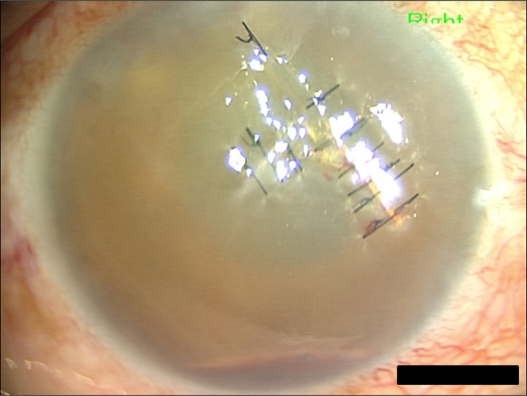
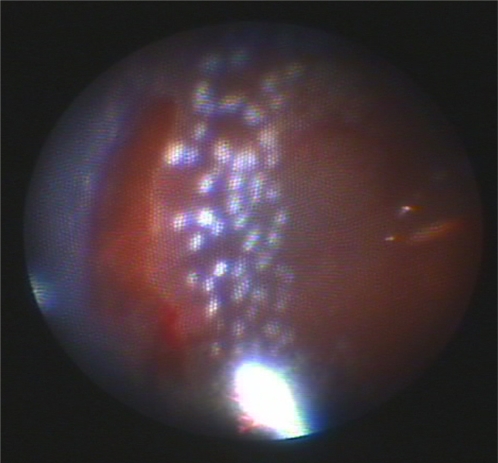
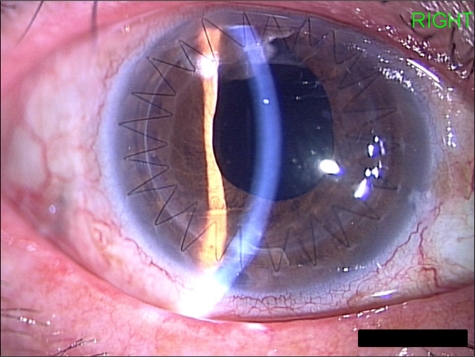
Case presentation: A 55-year-old Japanese woman was referred to our hospital with a perforating corneal and lens injury sustained with a muddy ferrous rod. Primary corneal sutures and lensectomy were performed immediately. Vitreoretinal surgery was required due to suspected endophthalmitis, vitreous hemorrhage, retinal detachment, dialysis and necrosis of the peripheral retina. Instead of conventional vitrectomy, endoscopy-guided vitreous surgery was performed with the Solid Fiber Catheter AS-611 (FiberTech, Tokyo, Japan) due to the presence of corneal opacity and the unavailability of a donor cornea. The retina was successfully attached with the aid of a silicon oil tamponade. Following removal of the silicon oil at 3 months after surgery, penetrating keratoplasty and intraocular lens implantation with ciliary sulcus suture fixation were performed. At 6 months after penetrating keratoplasty, the graft remained clear and visual acuity was 20/40.
Conclusion: Primary endoscopic surgery for vitreoretinal complications in eyes with perforating injury performed prior to penetrating keratoplasty appears to be advantageous in terms of avoiding damage to the corneal endothelium.
Keywords: emergency; foreign body; vitreoretinal surgery.
Figures
Similar articles
-
Comparative study of penetrating keratoplasty and vitreoretinal surgery with Eckardt temporary keratoprosthesis in ocular trauma versus non-trauma patients.Graefes Arch Clin Exp Ophthalmol. 2019 Nov;257(11):2547-2558. doi: 10.1007/s00417-019-04420-0. Epub 2019 Jul 30. Graefes Arch Clin Exp Ophthalmol. 2019. PMID: 31363832
-
Simultaneous Vitreoretinal Surgery and Penetrating Keratoplasty without a Keratoprosthesis or Endoscopy for Vitreoretinal Disease Associated with Corneal Opacity.Case Rep Ophthalmol. 2020 Mar 19;11(1):127-136. doi: 10.1159/000506589. eCollection 2020 Jan-Apr. Case Rep Ophthalmol. 2020. PMID: 32308614 Free PMC article.
-
Outcome of combined penetrating keratoplasty with vitreoretinal surgery for management of severe ocular injuries.Retina. 2003 Feb;23(1):48-56. doi: 10.1097/00006982-200302000-00008. Retina. 2003. PMID: 12652231
-
Penetrating keratoplasty surgery combined with vitrectomy after failing previous corneal surgery.Retina. 2003 Feb;23(1):41-7. doi: 10.1097/00006982-200302000-00007. Retina. 2003. PMID: 12652230
-
[Endoscopy-guided 20-G vitrectomy in severe endophthalmitis: Report of 18 cases and literature review].J Fr Ophtalmol. 2015 Dec;38(10):941-9. doi: 10.1016/j.jfo.2015.07.005. Epub 2015 Nov 10. J Fr Ophtalmol. 2015. PMID: 26563835 Review. French.
Cited by
-
Consolidation of Imaging Modalities Utilizing Digitally Assisted Visualization Systems: The Development of a Surgical Information Handling Cockpit.Clin Ophthalmol. 2020 Feb 27;14:557-569. doi: 10.2147/OPTH.S239339. eCollection 2020. Clin Ophthalmol. 2020. PMID: 32161441 Free PMC article.
-
Endoscopic vitreoretinal surgery: principles, applications and new directions.Int J Retina Vitreous. 2019 Jun 18;5:15. doi: 10.1186/s40942-019-0165-z. eCollection 2019. Int J Retina Vitreous. 2019. PMID: 31236288 Free PMC article. Review.
-
Endoscope-assisted vitrectomy in the management of retinal detachment with corneal opacity.Taiwan J Ophthalmol. 2017 Jul-Sep;7(3):164-167. doi: 10.4103/tjo.tjo_25_17. Taiwan J Ophthalmol. 2017. PMID: 29034157 Free PMC article.
-
23-gauge vitrectomy assisted by combined endoscopy and a wide-angle viewing system for retinal detachment with severe penetrating corneal injury: a case report.Clin Ophthalmol. 2011;5:1767-70. doi: 10.2147/OPTH.S25373. Epub 2011 Dec 14. Clin Ophthalmol. 2011. PMID: 22267909 Free PMC article.
-
Conjunctivitis in Novel Coronavirus Disease (COVID-19).Indian J Occup Environ Med. 2020 May-Aug;24(2):129-130. doi: 10.4103/ijoem.IJOEM_85_20. Epub 2020 Aug 19. Indian J Occup Environ Med. 2020. PMID: 33281386 Free PMC article. No abstract available.
References
-
- Eckardt C. A new temporary keratoprosthesis for pars plana vitrectomy. Retina. 1987;7:34–37. - PubMed
-
- Koenig SB, McDonald HR, Williams GA, Abrams GW. Penetrating keratoplasty after placement of a temporary keratoprosthesis during pars plana vitrectomy. Am J Ophthalmol. 1986;102:45–49. - PubMed
-
- Garcia-Valenzuela E, Blair NP, Shapiro MJ, et al. Outcome of vitreoretinal surgery and penetrating keratoplasty using temporary keratoprosthesis. Retina. 1999;19:424–429. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
